(UroToday.com) The 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023 was host to a bladder preservation strategies oral session. Dr. Elizabeth Plimack discussed the role of systemic therapy in bladder preservation for patients with muscle-invasive bladder cancer (MIBC).
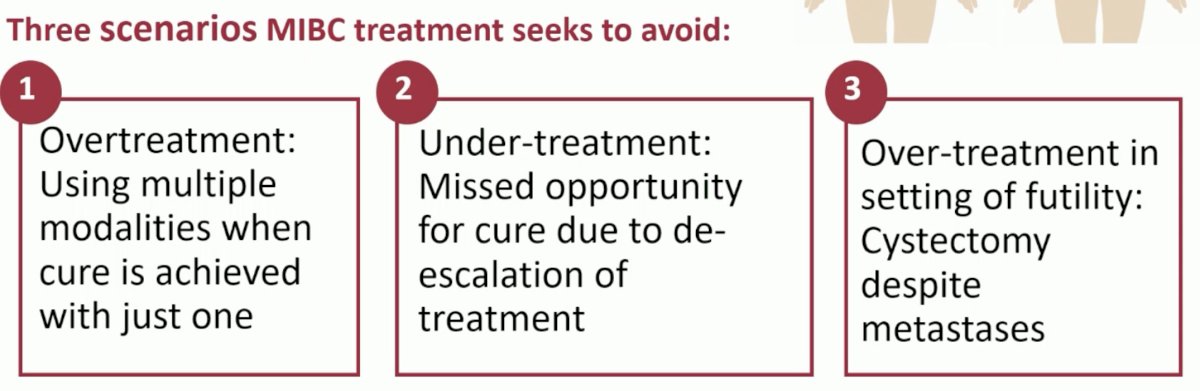
The overall goal of MIBC treatment is cure with the least possible quality of life detriment:
Following systemic therapy, there are currently three possible clinical scenarios for patients with MIBC, all of which end with surgery:
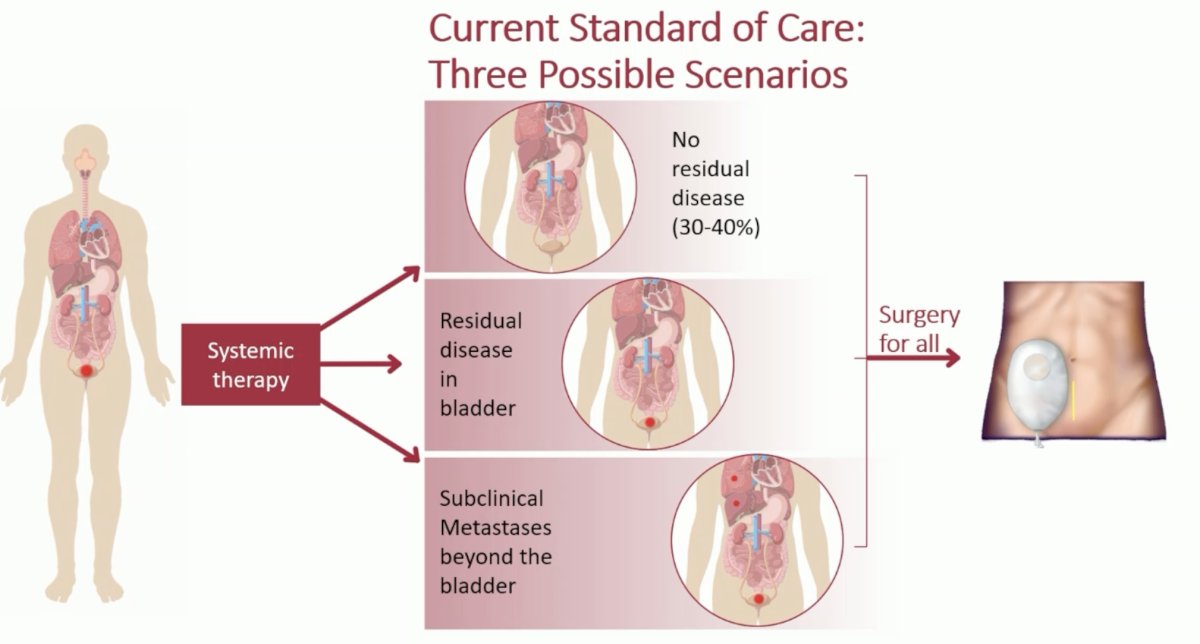
The current challenge remains to better identify those patients in each clinical scenario to guide a risk-adapted, escalation/de-escalation treatment approach.
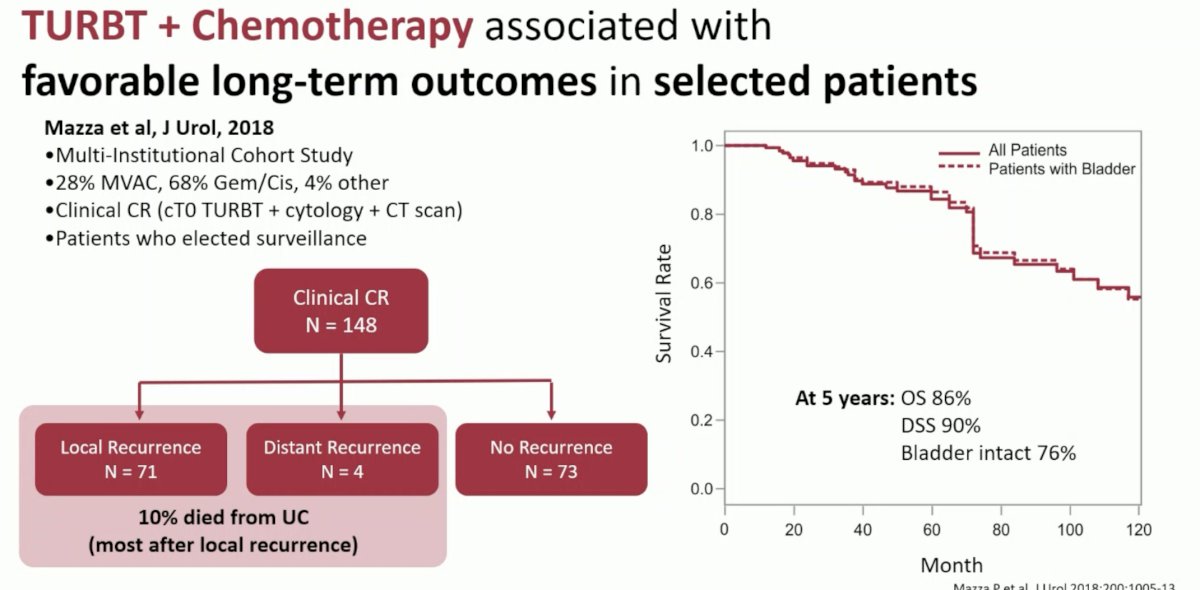
Can we achieve bladder preservation with systemic therapy alone? In 2018, Mazza et al. published the results of a multi-institutional cohort study of 148 patients with evidence of a complete clinical response, ascertained via TURBT, cytology, and CTR scan. Of these 148 patients, nearly half (73) had no recurrence during follow-up. Among the 75 (51%) who did recur, 71 had local recurrence, whereas only 4 had distant recurrences.1
Recently, there have been two ‘trials of allocation’ that have completed accrual and been presented/published: RETAIN (NCT02710734) and HCRN GU 16-257 (NCT03558087).
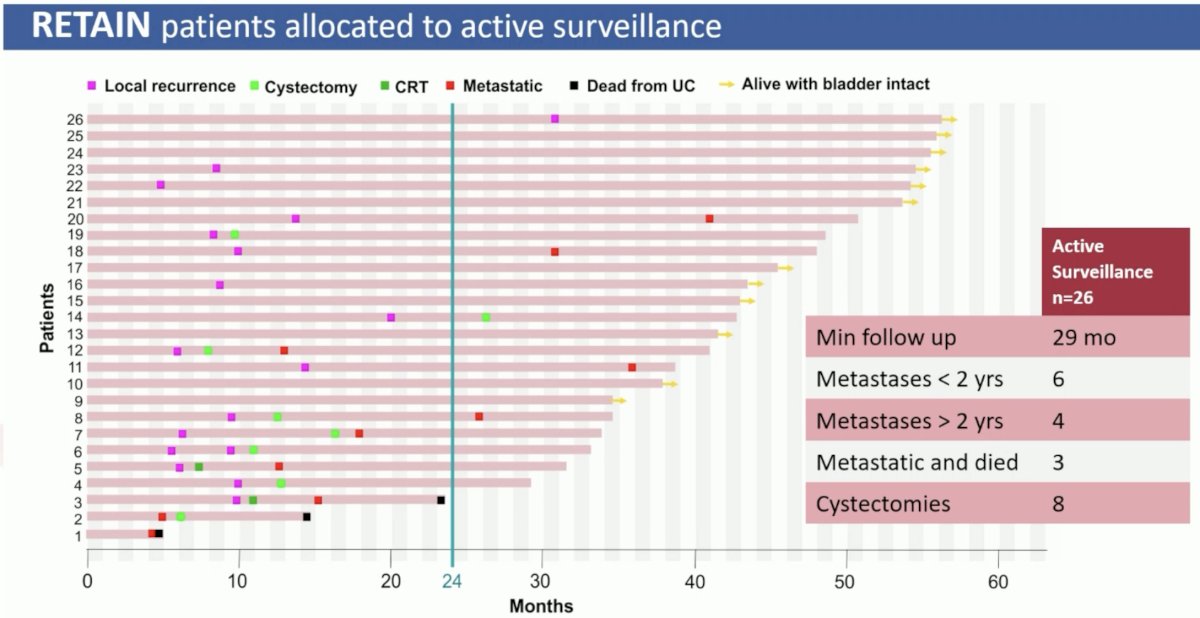
RETAIN included patients with cT2-3N0M0 bladder cancer who received accelerated MVAC followed by a second, re-staging TURBT. The treatment approach was risk adapted based on residual disease and mutational statuses:
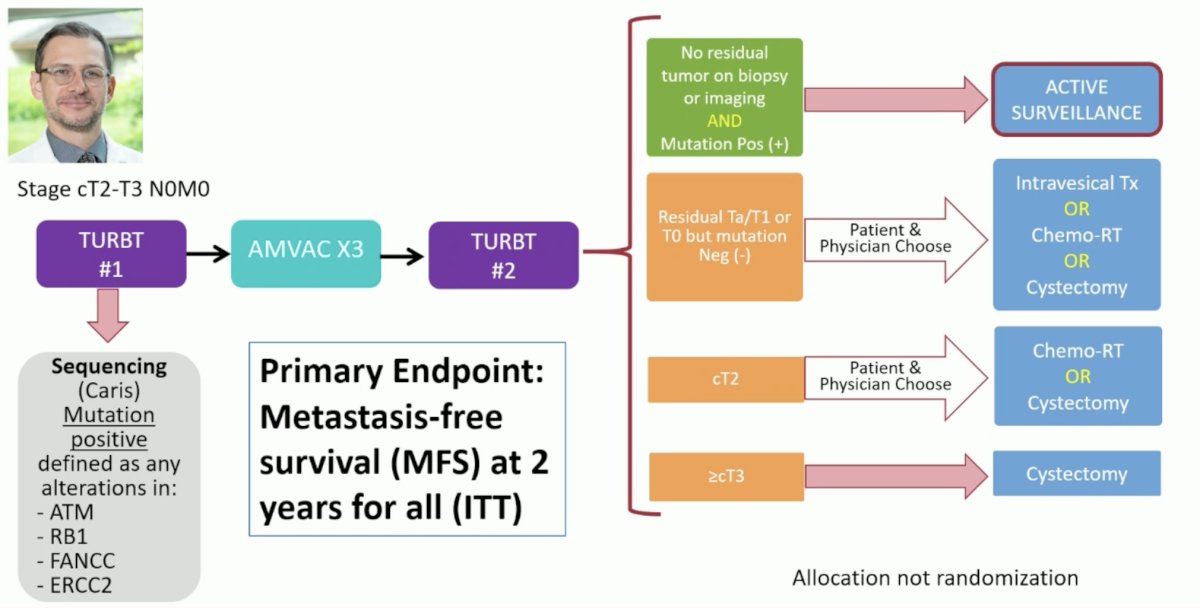
Patients with no residual disease on biopsy or imaging and a positive mutational status for ATM, RB1, FANCC, or ERCC2 were assigned to active surveillance. Those who were Ta-T1 or T0 with a negative mutational status were assigned to intravesical therapy, chemoradiotherapy, or cystectomy, following a shared decision-making process between the patient and physician.
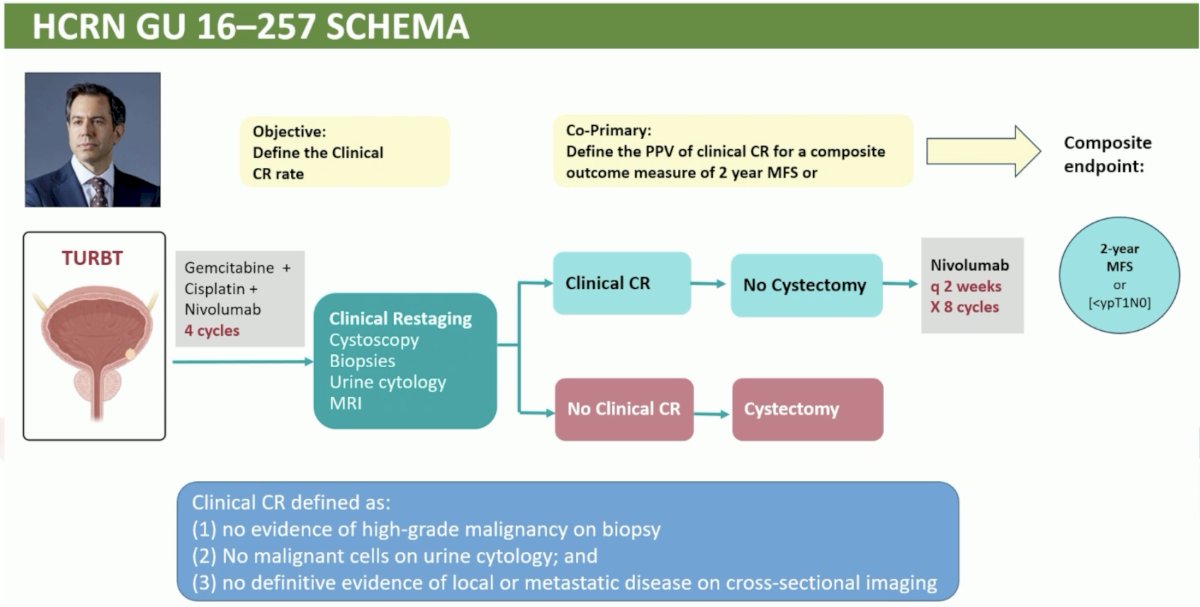
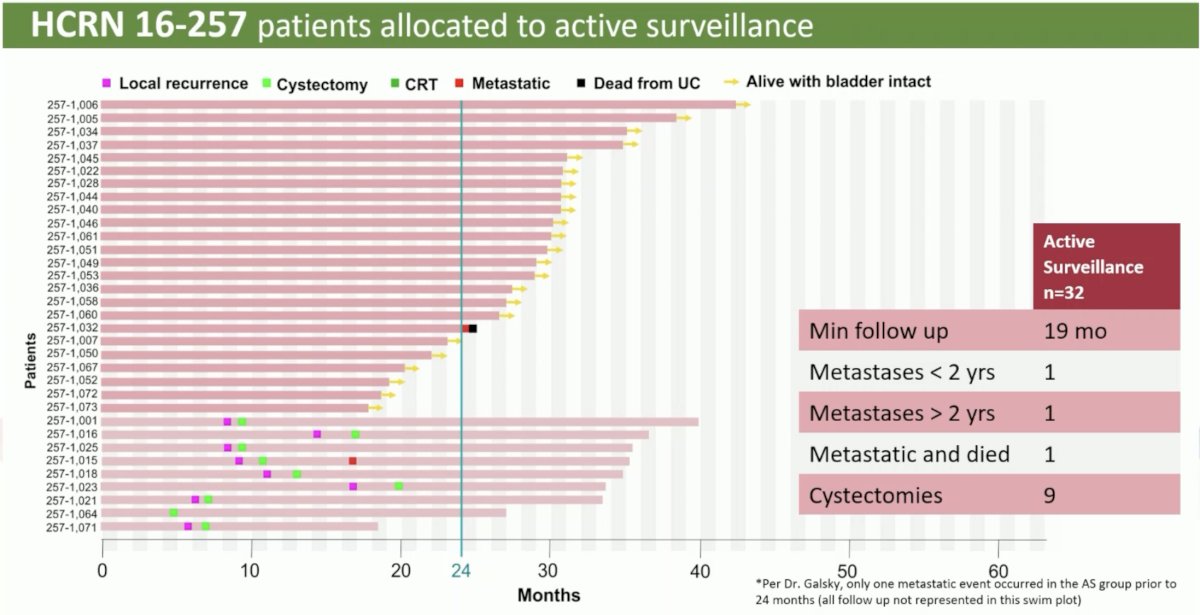
In HCRN GU 16-257, patients received nivolumab + gem/cis chemotherapy x 4 cycles, after which they were re-staged with cystoscopy + biopsy, urine cytology, and MRI. Those with evidence of a complete clinical response were recommended to forgo cystectomy and received adjuvant nivolumab every 2 weeks for a total of 8 cycles. The primary endpoint was 2-year MFS or <ypT1N0 in the patients with a complete clinical response.
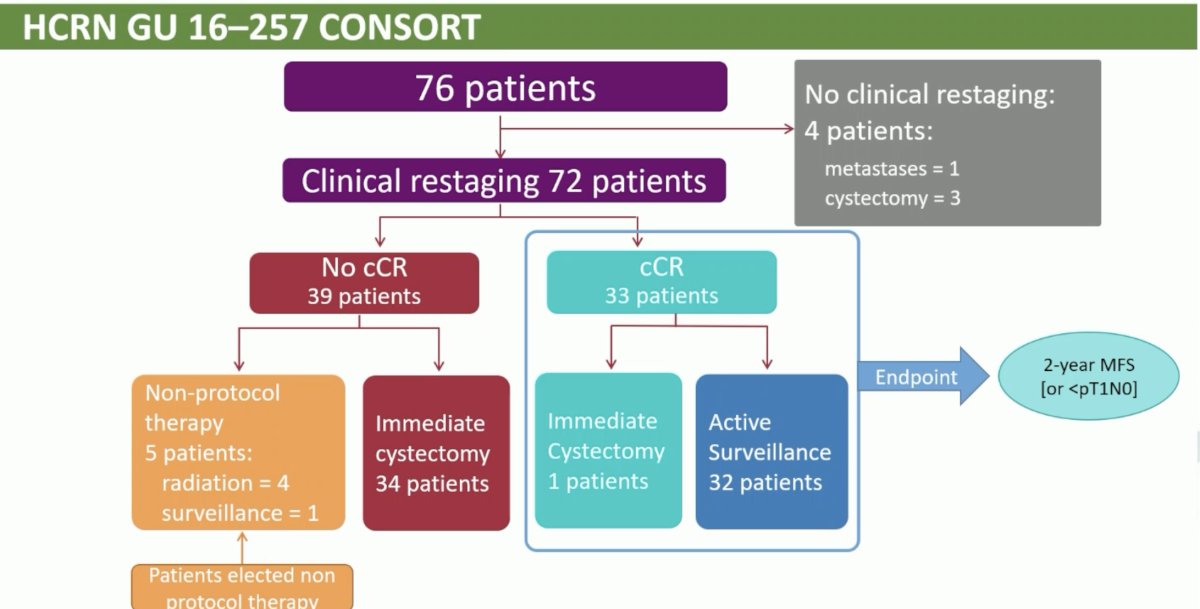
Among the 72 patients who were recruited and subsequently underwent clinical re-staging, 33 patients (46%) had evidence of a complete clinical response. One patient opted for immediate cystectomy, with the remaining 32 proceeding with active surveillance.
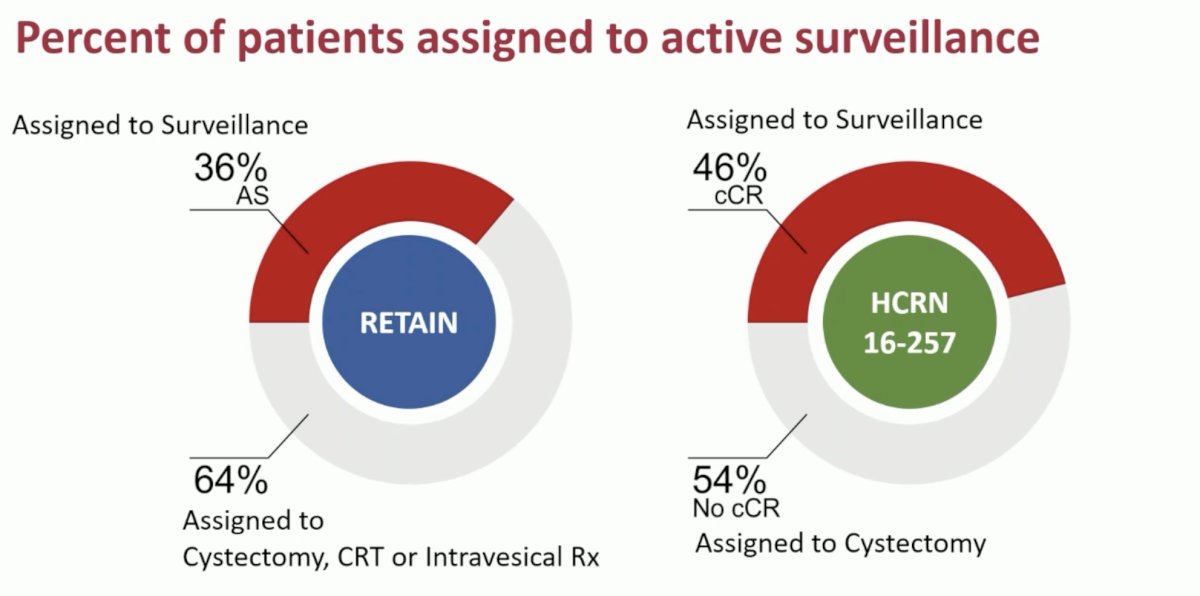
In the RETAIN trial, 36% of patients were selected for active surveillance (46% in HCRN GU 16-257).
In the RETAIN trial, 6/26 patients developed metastases in <2 years, with a further 4 developing metastases after 2 years. 3 of these 10 patients have died of their metastatic disease. 8/26 patients underwent a cystectomy during a minimum follow-up of 29 months.
In HCRN GU 16-257, 1 patient developed metastases each before and after 2 years follow-up. Of these 2, 1 had died of their metastatic disease. 932 patients underwent a cystectomy during a minimum follow-up of 19 months.
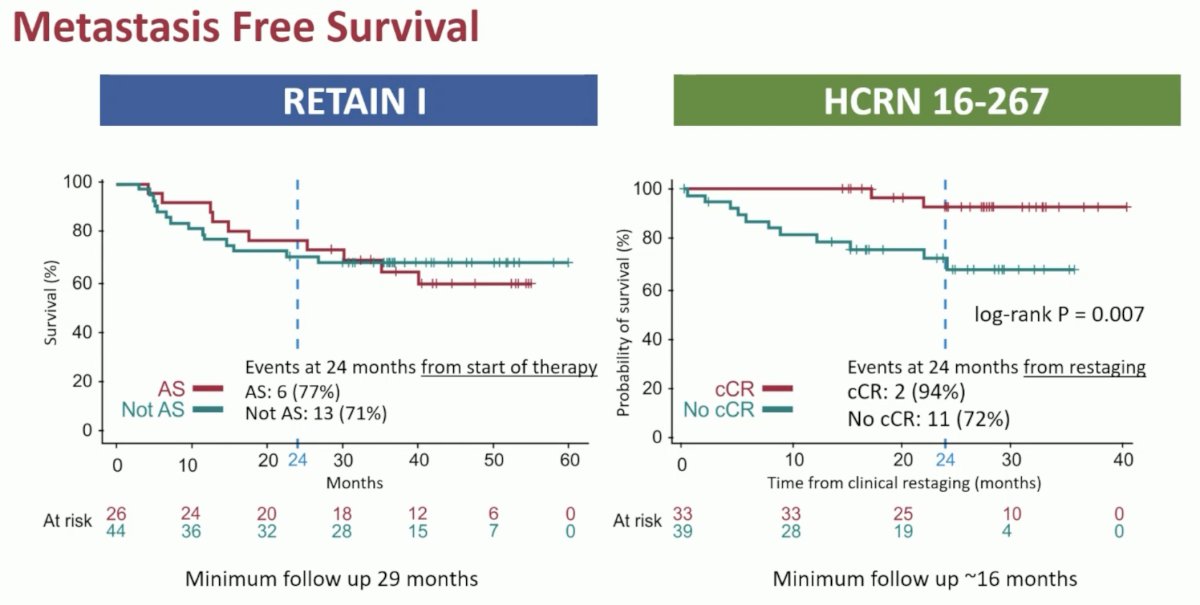
The metastasis-free survival (MFS) for each trial is summarized below. In the RETAIN trial, the MFS was similar for patients in the ‘AS’ and ‘not AS’ arms. These results suggest that the underlying biology, as opposed to treatment chosen, may be driving clinical outcomes in this setting. In HCRN GU 16-257, patients with a complete clinical response had superior MFS compared to those without, which provides additional reassurance regarding the suitability of the bladder-sparing approach for these patients.
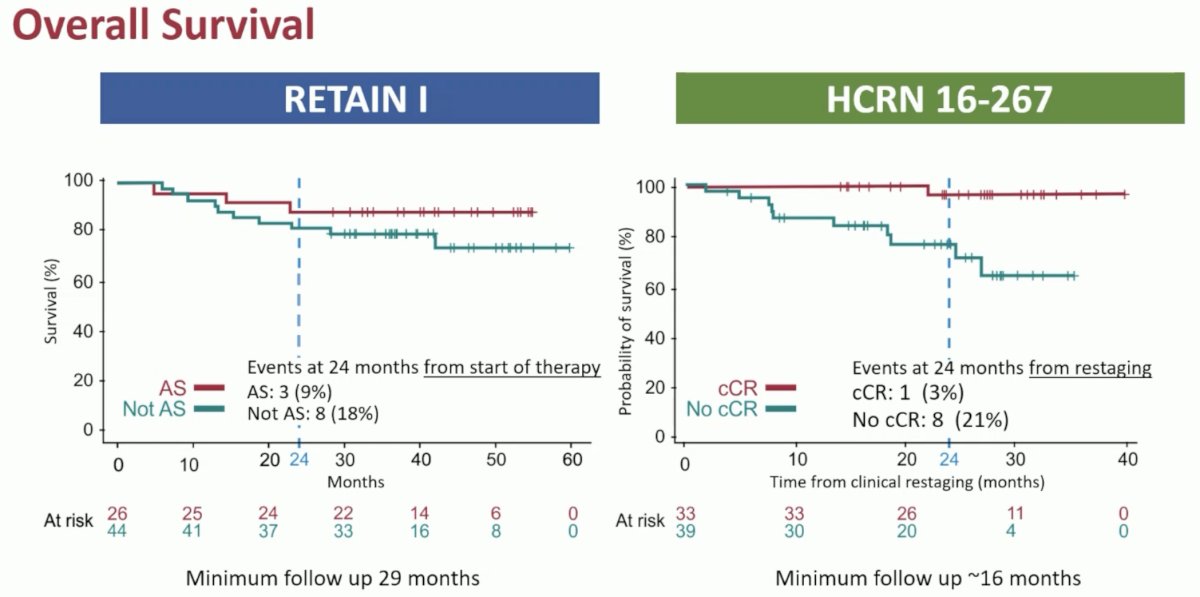
Similar trends were observed for overall survival:
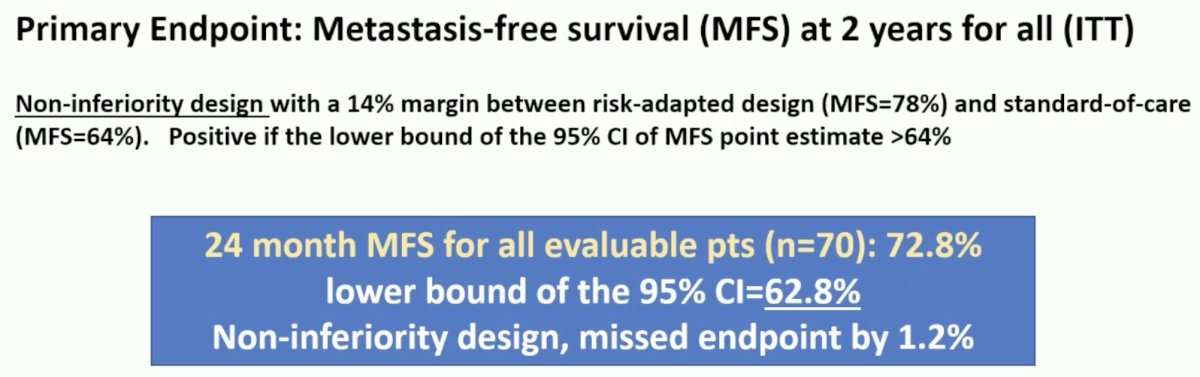
Overall, RETAIN failed to meet its primary endpoint of MFS at 2 years for all patients in the intent to treat population.
Conversely, HCRN GU 16-257 met its primary endpoint with 30/32 clinical complete response patients reaching 24 months follow-up without evidence of metastases. The ‘positive predictive value’ as such was 97% which exceeded the pre-determined cut-off of 80%.
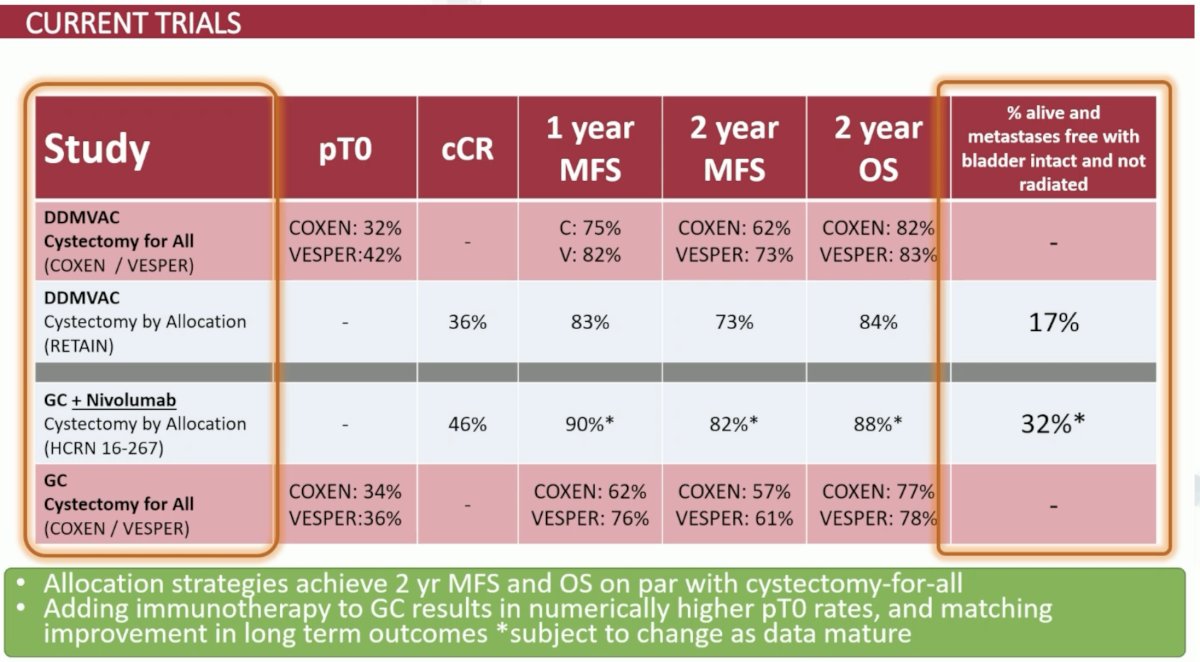
When put in context, the results of RETAIN and HCRN GU 16-257 compare favorably to those of historic trials of neoadjuvant ddMVAC or gem-cis followed by cystectomy for all patients. Notably, 17% of patients in RETAIN and 32% of patients in HCRN GU 16-257 remained metastasis-free with an intact, non-radiated bladder at the end of follow-up, compared to none in the other trials (all had planned cystectomy).
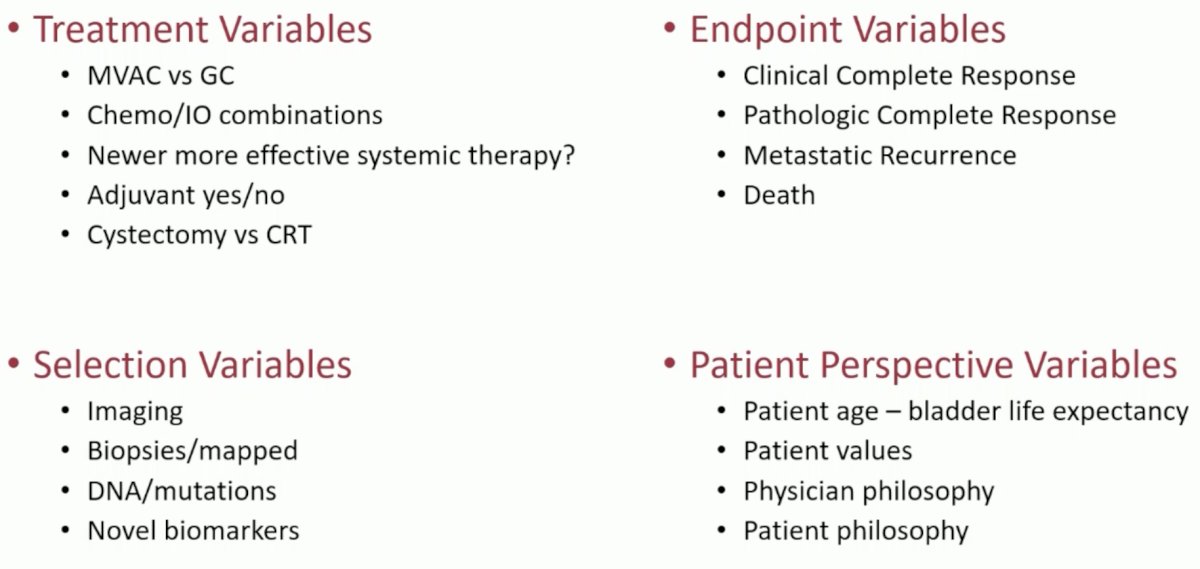
When considering trial design in this disease space, there are numerous variables to consider, pertaining to treatment choice, study endpoints, treatment selection, and patient perspectives.
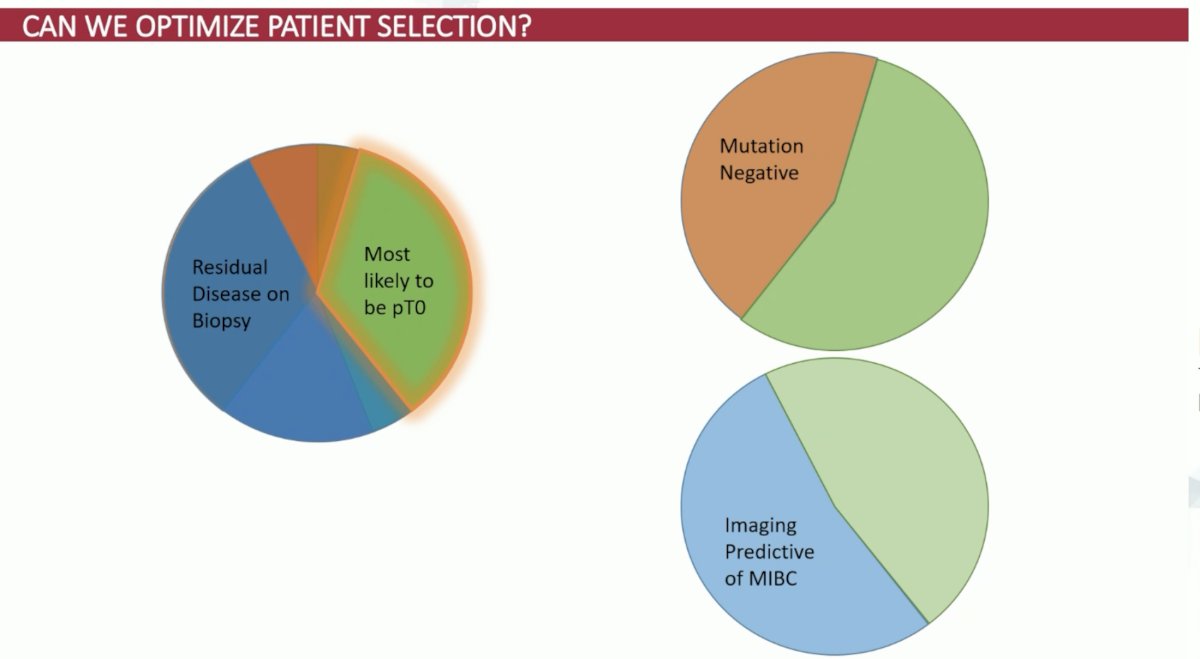
What variables are currently available for treatment selection in clinical practice?
- Pathology mapped biopsies
- Among patients without tumor on biopsy, 52% had evidence of tumor present at surgery. As such, this test under-estimate disease in half of patients
- Among those with NIMBC or MIBC at biopsy, 97% had tumor present at surgery

- Biomarker NGS mutations in ATM, RB1, ERCC2, and FANCC
- For those with any of these mutations, 52% had evidence of tumor present at surgery
- Among those with no mutations, 86% had evidence of tumor present at surgery
- As such, this test may be used to ‘rule out’ those who are unlikely to have absent tumor at surgery
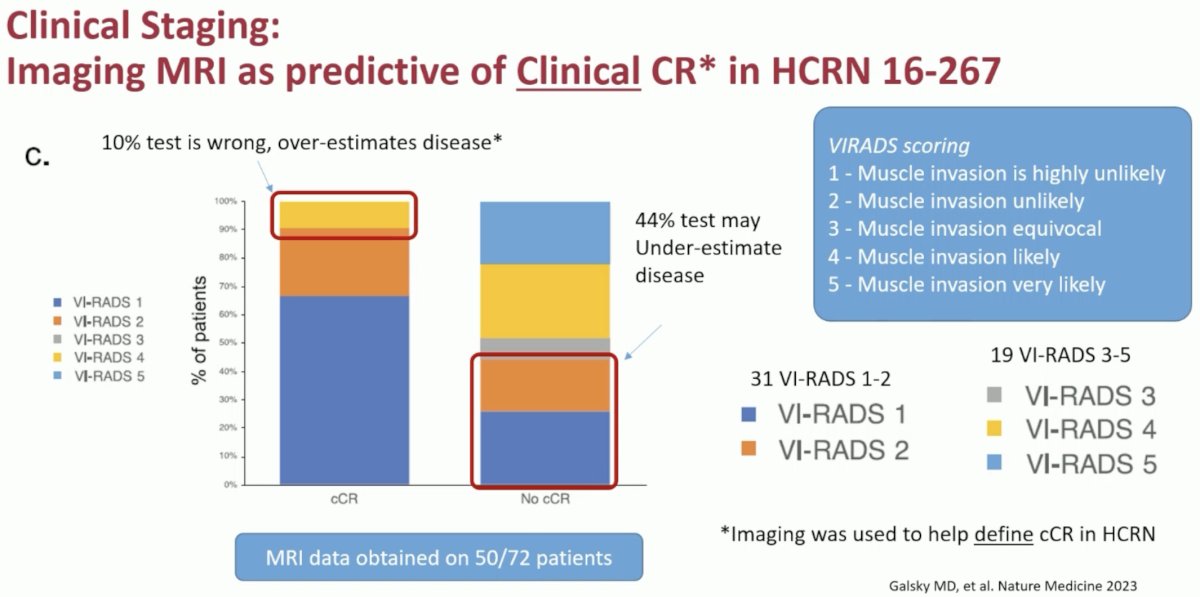
- MRI
- While used in HCRN GU 16-257, this test may underestimate disease in 44% of patients and in Dr. Plimack’s opinion, is not yet ready for primetime for this selection process
One possible treatment selection paradigm in the immediate future may include combining these three factors to optimize patient selection in this setting.
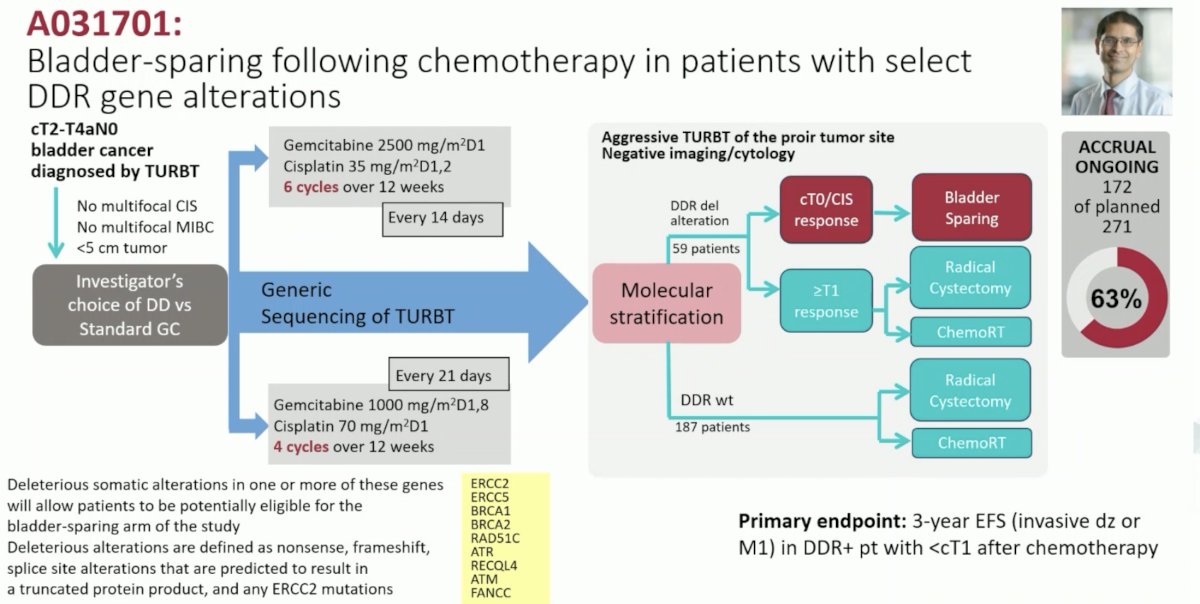
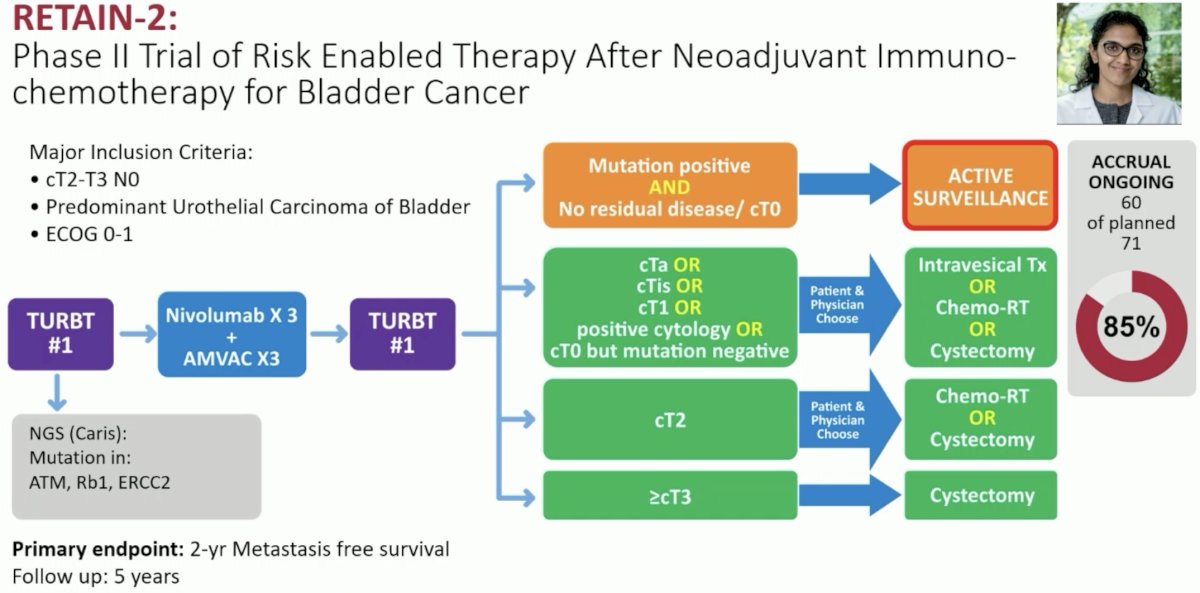
Currently ongoing trials in this disease space include ALLIANCE A031701 (NCT03609216) and RETAIN-2 (NCT04506554), which is adding neoadjuvant nivolumab to accelerated MVAC.
Dr. Plimack concluded as follows:
- We need to aim to balance quality of life with cure
- Not every MIBC bladder needs to be/should be removed or radiated, sparing associated side effects
- Systemic therapies, imaging, and biomarkers will only improve our ability to cure with systemic therapy alone
- We should seek to avoid under-treatment and over-treatment to tailor the right amount of therapy to each person
Presented by: Elizabeth R. Plimack, MD, MS, Professor, Department of Hematology/Oncology, Deputy Director, Fox Chase Cancer Center, Philadelphia, PA
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Society of Medical Oncology (ESMO) Annual Meeting, Madrid, Spain, Fri, Oct 20 – Tues, Oct 24, 2023.
References: