Radical cystectomy is the preferred definitive treatment for muscle-invasive bladder cancer (MIBC). Neoadjuvant chemotherapy is indicated in patients with clinical stage T2-T4 N0 M0. Induction chemotherapy is mandated in patients with positive node disease but with localized MIBC. Ideally, every patient planned for radical cystectomy should receive perioperative chemotherapy and optimal surgery with an extensive lymph node dissection. Neoadjuvant chemotherapy has been proven to add a significant survival benefit.
The European Association of Urology (EAU) and the European Society for Medical Oncology (ESMO) guidelines state that neoadjuvant chemotherapy should be offered to patients with T2-T4a N0M0 bladder cancer, and cisplatin-based combination chemotherapy should always be the regimen that is used (grade A evidence). In contrast, adjuvant cisplatin-based combination chemotherapy should be given to patients with pathological T3/4 and N+ disease if no neoadjuvant chemotherapy has been given. However, the guidelines also state that in patients who are ineligible for cisplatin-based chemotherapy, neoadjuvant chemotherapy is not recommended. Importantly, the American Society of Clinical Oncology (ASCO) guidelines note that they support neoadjuvant chemotherapy in cisplatin-ineligible patients if the goal is to downstage surgically unresectable tumors. Unfortunately, the proportion of patients who are unfit for cisplatin chemotherapy is quite high, at around 40-50%.
In 2011 criteria to define cisplatin “unfit” patients were formed.6 These include:
- WHO or ECOG performance status 2 or Kranofsky of 60-70%
- Creatinine clearance <60 ml/min
- Common Terminology Criteria for Adverse Events (CTCAE) v4 grade >=2 audiometric hearing loss
- CTCAE v4 grade >=2 peripheral neuropathy
- New York Heart Association Functional Classification (NYHA) class III heart failure
Four total cycles of platinum-based first-line chemotherapy have been shown to be adequate to treat advanced urothelial carcinoma. The omission of additional cycles might help avoid unnecessary toxicities and facilitate a better transition to second-line treatment and switch maintenance therapy.
Second line chemotherapy has limited activity in metastatic urothelial carcinoma. A meta-analysis of studies investigating single-agent or doublet second-line chemotherapy in advanced urothelial cancer had shown that the 2nd line chemotherapy had very limited activity, with third line data being scarce.7 It is still not clear what the role of chemotherapy would be following immunotherapy.
The RANGE is a randomized, double-blind phase 3 study, compares Ramucirumab (a fully human monoclonal antibody developed for the treatment of solid tumors) plus docetaxel vs. placebo plus docetaxel in patients with locally advanced metastatic urothelial carcinoma after platinum-based therapy.8 The results demonstrated a clear benefit for the Ramucirumab+ docetaxel arm with progression-free survival of 4.07 months vs. 2.76 months, and objective response rate of 24.5% vs. 14%, with no significant difference in the adverse events profile.
In a study comparing sequencing of immunotherapy before chemotherapy to chemotherapy before immunotherapy, and then followed again by chemotherapy, the response rate was 64% for the chemotherapy-immunotherapy-chemotherapy sequence, vs. 21% in the immunotherapy- chemotherapy sequence.9
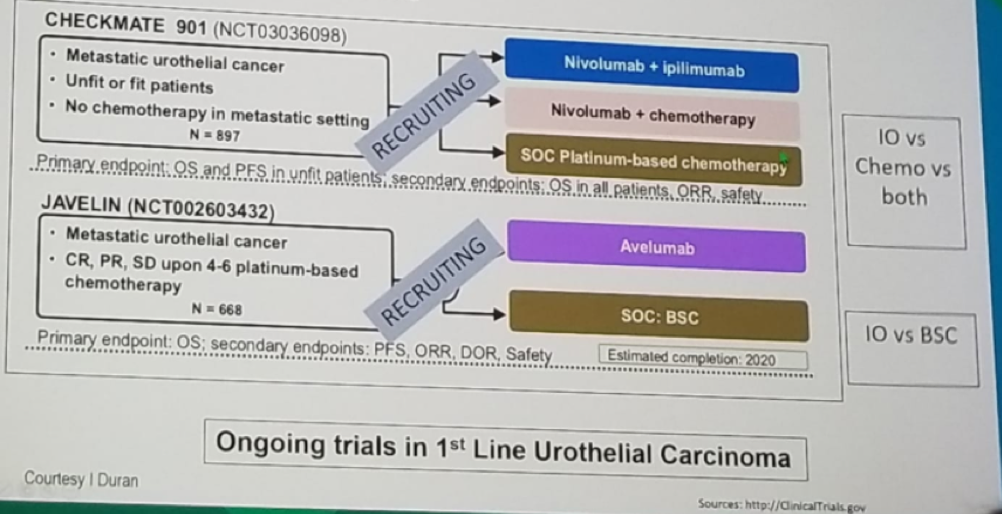
In summary, chemotherapy remains the standard of care in neoadjuvant setting and first-line setting for metastatic medically unfit patients. The long-term survival with chemotherapy is 10-15% at 3-5 years (first line therapy), and 11% at two years (for second-line therapy). Chemotherapy should be incorporated into the treatment paradigm together with immunotherapy. There are currently only preliminary results showing that immunotherapy has promising downstaging potential. Further studies are underway, including combinations of immunotherapy with chemotherapy (Figure 1). Lastly, it is important to remember that in these specific patients, offering enrollment in clinical trials is part of helping these patients and is mandated to advance our knowledge.
Figure 1 – Chemotherapy and immunotherapy Combination Trials:

Presented by: Maria De Santis, MD, Berlin, DE
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter: @GoldbergHanan at the 2018 European Society for Medical Oncology Congress (#ESMO18), October 19-23, 2018, Munich Germany
References:
- Sternberg et al. Cancer 64: 2448-2468, 1989
- Sternberg et al. Eur J. Cancer, 42: 50-54, 2006
- Plimack et al. J Clin Oncol 2014
- Von der Masse H et al. JCO 2015
- Hussain et al. BJC 91:844-849, 2004
- Galsky et al. J Clin Onco 2011; 29:2432-2438
- Raggi D et al. Ann Oncol 2016
- Petrylak et al. Lancet 2017
- Szabados et al. Eur Urol 2018