BCG is thought to work via immune-mediated pathways, through secretion of the inflammatory cytokine, TH-1 response, and recruitment of cytotoxic T cells + natural killer (NK) cells. BCG failure is quite common with high-risk (Ta or T1 high grade or CIS) bladder cancer recurrence occurring after transurethral resection of bladder tumor (TURBT) with BCG therapy in 66% of cases, with a rate of 25% progression.1 Approximately 78% of the recurrences have associated CIS.
Radical cystectomy is the current standard for BCG unresponsive disease. It results in excellent survival, (90% cancer-specific survival rate). Delaying radical cystectomy reduces the chances of cure from this disease. The earlier radical cystectomy is performed, the better. However, in some NMIBC patients, radical cystectomy is an overtreatment. Radical cystectomy has major negative implications for the patient, including functional and cosmetic implications. Unfortunately, to date, there is no other effective salvage intravesical therapy in BCG unresponsive patients. Only Thiotepa and Valrubicin have been used, and they have been approved since 1959. Other treatments have been examined as well, as detailed in table 1.
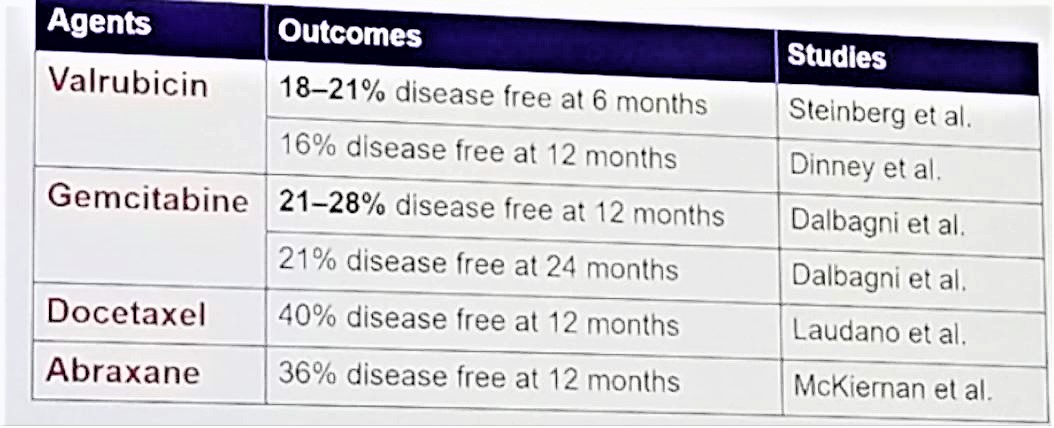
Table 1- Other treatments for NMIBC:
Checkpoint inhibitors are expressed in NMIBC. The Highest expression of PD-L1 is in CIS. There are approximately 5% of cells with PD-L1 before BCG therapy, and this rises 15-20 times with CIS recurrence after BCG treatment.2 There is a particularly high PD-L1 expression in BCG-induced granulomata of patients with recurrence after BCG. There is emerging data supporting a potential role for checkpoint inhibitors in NMIBC. There is increased expression of PD-1 on tumor infiltrating lymphocytes (TIL) after BCG therapy.3 TIL expression of PD-1 is correlated with tumor expression of PD-L1. There is an increase of PD-1 positivity in 67% of tumors after BCG relapse.4
Dr. Shariat continued and described what are the ideal expectations from a “bladder salvage” therapy in BCG unresponsive NMIBC. This therapy needs to be easier to use than to perform a radical cystectomy, it cannot be more toxic than radical cystectomy (preferably it needs to be less toxic), it has to have clinical acceptable efficacy, have a very low risk of missing the “window of opportunity”, with low risk of progressing to invasive muscle disease, and minimal delay in receiving radical cystectomy if the therapy fails. Lastly, it should not increase the complications of radical cystectomy, in case it fails.
Dr. Shariat then moved on to discuss the results of the Keynote 057 study of pembrolizumab for BCG unresponsive CIS +/- papillary high-grade bladder cancer. According to Dr. Shariat, the authors of this study used the right definition of BCG failure, occurring after adequate BCG treatment (BCG induction of 6 weeks plus at least one BCG maintenance instillation), and defined as the occurrence of high-risk disease at the six months timepoint after diagnosis for high-risk tumor. BCG unresponsive disease is defined as a BCG refractory disease + BCG relapsing within six months of last BCG therapy.
The keynote 057 trial demonstrated that pembrolizumab therapy was not more toxic than radical cystectomy with similar adverse effects in general (63-64%), grade 3-5 adverse events (13%), and lower mortality (1% vs. 3-5%) when compared to radical cystectomy. The clinical efficacy was quite acceptable, with 38.8% complete response rates at three months, and 75% durable response (31% at last follow-up). There was also a very low risk of missing the “window of opportunity” with 0% progression to invasive muscle disease, and all failures remaining NMIBC! All 85% of failures occurred at three months with no resulting delay to radical cystectomy. Lastly, the complications of radical cystectomy were not increased as a result of this treatment.
The major limitations of the Keynote 057 include its single-arm trial design, but this is acceptable in this setting. This is still only an interim analysis, and we need the 12 months data. In this trial, there is a possibility for detection bias, as no enhanced optical imaging in cystoscopy were used, and this has been proven to detect up to 30% more CIS. Lastly, most patients in this trial refused radical cystectomy, as opposed to not being ineligible for this procedure. However, this still represents an unmet need.
Bladder cancer is generally a heterogeneous disease, and not all tumors that recur after BCG therapy are the same. Many NMIBC tumors cluster with muscle-invasive bladder cancers. The key is understanding the various risk categories of tumors that patients can recur with following BCG therapy.
The combination of Pembrolizumab with BCG is the next step that needs to be studied. This combination increases the number and activity of TIL (CD8 and T cells), it elicits tumor growth inhibition, prolongs survival, and is more effective than either agent alone. The Keynote 676 is a phase 3 trial analyzing the effect of pembrolizumab and BCG in the induction of patients after BCG failure. In addition to this, there are other trials analyzing the effect of other immune checkpoint inhibitors in NMIBC, as can be seen in table 2.

Table 2 – Other immune checkpoint inhibitors analyzed in NMIBC:
Finally, other immunomodulatory agents are being assessed. These include ALT 803 (IL-15 agonist), iFNA gene therapy, and an oncolytic virus. The future holds great promise in the development of novel treatments for NMIBC.
Presented by: Shahrokh F. Shariat, MD, Department of Urology, Comprehensive Cancer Center, Medical University of Vienna, Austria
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the 2018 European Society for Medical Oncology Congress (#ESMO18), October 19-23, 2018, Munich Germany
Further Related Content:
Ronald De Wit, MD, Ph.D. Presentation Pembrolizumab for High-Risk Non–Muscle Invasive Bladder Cancer Unresponsive to BCG: Phase 2 Keynote-057 Trial
References:
1. Herr et al. J Urol 2010
2. Inman et al. Cancer 2007
3. Boorjian et al. Clin Cancer Res 2008
4. Fukumoto et al. J Surg Oncol 2018