(UroToday.com) In the fifteenth and final session of the 2022 International Kidney Cancer Symposium (IKCS): Europe meeting focusing on questions of therapeutic management dilemmas, Dr. Vasudev considered the potential role of withholding therapy as a treatment strategy in patients with advanced and metastatic renal cell carcinoma (mRCC) who are receiving immunotherapy based treatment regimes. This is premised on the notion that the combination of anti-PD(L)-1 with anti-CTLA4 therapy can have durable disease control but often comes at a cost of patient-borne treatment toxicity, financial costs to the patient and health care system, and other potentially detrimental effects. Therefore, if we could de-escalate therapy without compromising outcomes, this may offer a significant benefit over our current treatment paradigm.
Examining the current treatment schedule for a patient receiving nivolumab and ipilimumab for mRCC, Dr. Vasudev suggested that there are potentially a number of different was that we may consider treatment de-escalation:
1. Do we need to give combination therapy with ipilimumab upfront?
2. Could we give ipilimumab less frequently?
3. Could we change the number of doses or dose intensity?
4. Could we safely stop therapy and, if so, when?

Addressing the first of these (do we need to administer ipilimumab upfront with nivolumab), he highlighted three similar, but not identical, trials: OMNIVORE, TITAN-RCC, and HCRN-GU-260. In each case these trials used an initial nivolumab monotherapy induction followed by treatment stratified by response: patients who had partial or complete responses continued on nivolumab monotherapy while those with stable or progressive disease had intensification with the addition of ipilimumab. Unfortunately, while nivolumab monotherapy shows activity (with approximately a 30% objective response rate), duration of response and progression-free survival appear to be inferior as do complete response rates when compared with a combination approach. Further, there is a relatively poor ability to “rescue” with the addition of ipilimumab. Thus, he concluded that the combination approach remains the standard of care, in the absence of a way to select patients for response.
An alternative approach to potentially de-escalate therapy is a modification of the treatment schedule: PRISM is a randomized comparison of administering ipilimumab every 12 weeks, instead of the usual every three 3 weeks.

This less frequent ipilimumab dosing regime appears to be more tolerable (adverse events decreased from 53% to 33%; OR 0.43, 95% CI 0.25-0.72), without apparently affecting efficacy, based on data presented at ESMO 2021.
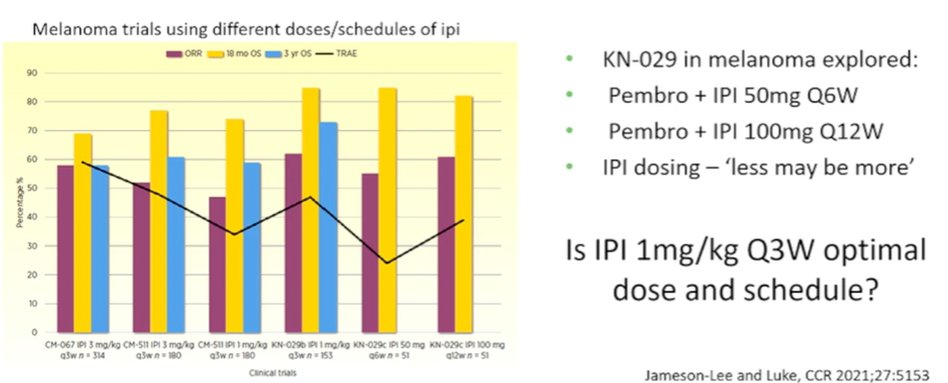
An alternative approach is decreasing the dose of ipilimumab. Citing data from both mRCC as well as from melanoma, he suggested that, in the short term, 1 mg/kg of ipilumumab appears similarly efficacious to 3 mg/kg. However, he asked whether we can do better than this. Citing data from the melanoma literature, alternative doses and schedules were explored with a suggestion of retained efficacy and decreased toxicity for patients receiving lower doses (50 mg every 6 weeks) or less frequently (100 mg every 12 weeks).
Further, Dr. Vasudev considered when we may safely stop therapy. The current two year cut-off was defined arbitrarily. In contrast, he cited data from high-dose IL-2 treatment showing that an initial treatment period can be followed by prolonged durable complete response while off therapy in some patients. While the data is post hoc from CheckMate 214, those patients who had to stop treatment early as a result of toxicity did not appear to have worse long-term survival outcomes. Treatment-related toxicity may be a marker of a good, long-term oncologic outcome and, in fact, he suggested that we may be over-treating many patients by requiring the prolonged durations of therapy. Further, a conditional survival analysis of patients from the CheckMate 214 trial demonstrated that a very large proportion of those who have a response at three years will maintain this to five years. However, it is not clear whether this is because of or in spite of maintenance therapy.
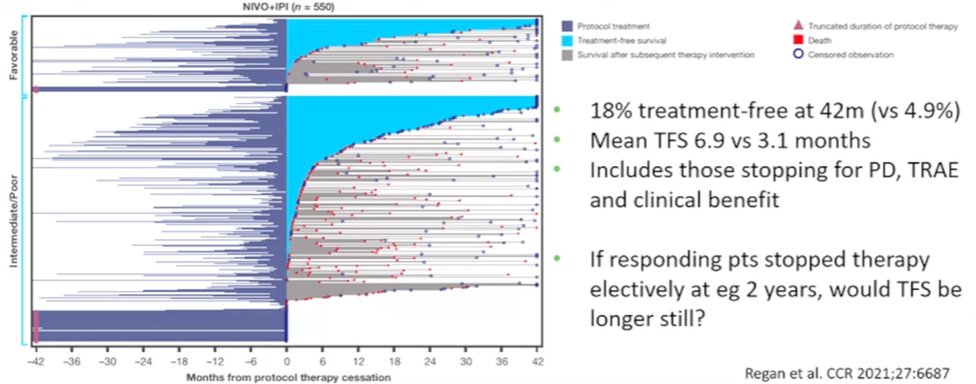
Dr. Vasudev suggested that our ultimate goal ought to be to provide patients with survival time off therapy. Thus, recent work looking at treatment-free survival among patients in the CheckMate 214 trial is of interest: there is a subset of patients who have a prolonged treatment free survival. He suggested that if patients who were responding electively stopped therapy at 2 years, we may be able to further increase this treatment free survival for many.
To better assess this, the REFINE trial is opening in the UK as a basket trial with an RCC cohort as the first to open. Among patients receiving standard of care immune checkpoint inhibitor therapy, patients will be randomized to a standard dosing schedule or extended interval. In the context of RCC, this will mean a randomized comparison of nivolumab maintenance every 4 weeks or every 8 weeks.
Summarizing, Dr. Vasudev concluded that, while active, single agent nivolumab is less favourable than combination therapy as first-line treatment so the combination should remain standard of care. However, there are numerous available opportunities to reduce the burden of treatment for patients receiving nivolumab and ipilimumab.
Presented by: Naveen Vasudev, MBChB, MRCP, PhD, Academic Medical Oncologist, University of Leeds, School of Medicine, UK