Up to 50% of patients with MIBC die of their disease. The introduction of neoadjuvant chemotherapy (NAC) has been associated with a 5-8% absolute improvement in the overall survival rates for patients with MIBC.1 Emergence of IO-based approaches in the adjuvant space, in particular with nivolumab in the CheckMate-274 trial, have led to improvements in 6-months DFS from 60% to 75%, with a median rPFS improvement of 9.2 months.2 However, overall survival benefits in this cohort remain unclear.
Current guidelines, highlighted by the EAU guidelines, recommend neoadjuvant chemotherapy given the proven 5-8% OS benefits. With regards to adjuvant therapy, the EAU guidelines recommend offering “adjuvant cisplatin-based chemotherapy to patients with pT3/4 and/or pN+ disease if no NAC. Offer adjuvant nivolumab to selected patients with pT3/4 and/or pN+ disease not eligible for or who declined adjuvant cisplatin-based chemotherapy”.
While neoadjuvant and adjuvant therapies have attractive survival benefits, it is important to highlight that not all patients benefit equally and “one size does not fit all”. When considering systemic therapy options in patients with MIBC, we need to adopt a more parsimonious, risk-adapted approach in MIBC, considering the following domains:
- Eligibility
- Response rates
- Complications
- Tools to guide decision-making
- Considerations for our patients
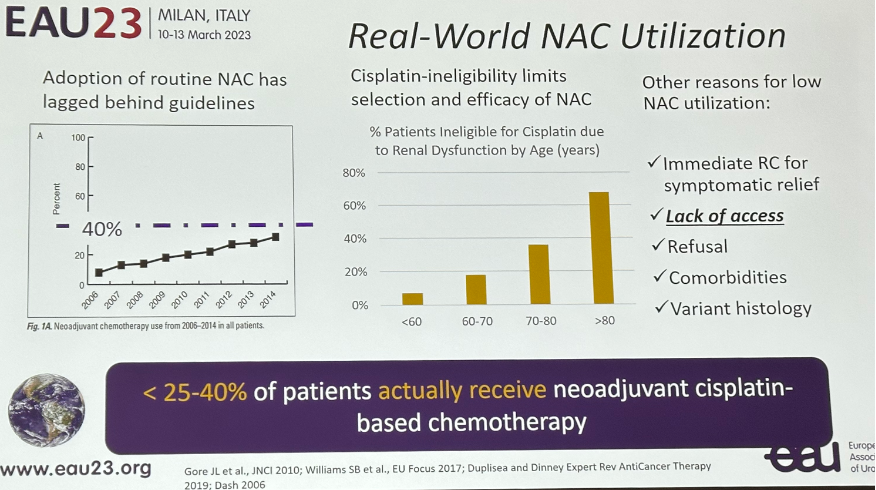
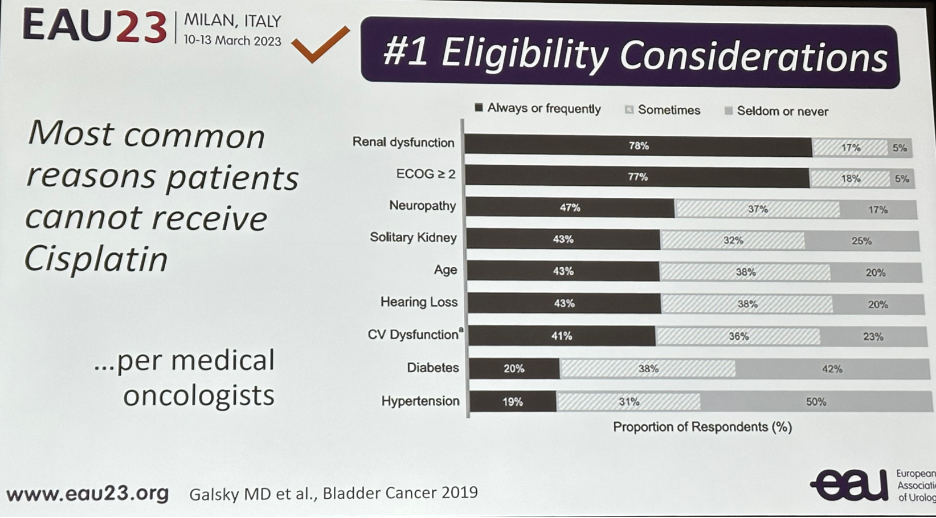 This is reflected in the real-world NAC utilization rates which remain at only 25-40% of all eligible candidates. This is likely multifactorial in etiology with causes including:
This is reflected in the real-world NAC utilization rates which remain at only 25-40% of all eligible candidates. This is likely multifactorial in etiology with causes including:- Cisplatin ineligibility
- Need for immediate radical cystectomy for symptomatic relief
- Refusal
- Comorbidities
- Presence of variant histology
 In addition to cisplatin eligibility, the second consideration here is whether all MIBC patients respond to cisplatin. While we highlighted a pCR rate of up to 40%, it does mean that at least 60% of patients do not achieve a pCR.
In addition to cisplatin eligibility, the second consideration here is whether all MIBC patients respond to cisplatin. While we highlighted a pCR rate of up to 40%, it does mean that at least 60% of patients do not achieve a pCR.
The concern here is that in non-responders, we risk delaying definitive treatment and subsequent disease progression. If we take a step back and think about the usual timeline for such patients from NAC to radical cystectomy, patients undergo a TURBT then receive NAC 6+ weeks later, then another 8-12 weeks for the NAC which varies in duration based on the regimen, and then recover for 4-6 weeks before they get the cystectomy. When we consider that delays of >12 weeks to radical cystectomy increase the risks of non-organ confined disease, LN metastases, lymphovascular invasion, cancer-specific mortality, and all-cause mortality, a delay of 6 months in non-responders is highly significant.
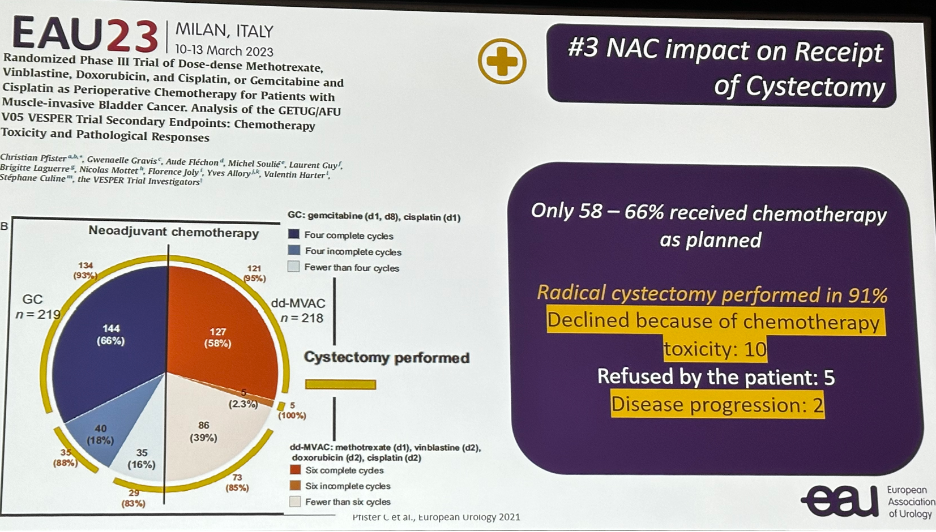
The third consideration is: how well is NAC tolerated and what is its impact on receipt of cystectomy? In the VESPER trial of neoadjuvant ddMVAC versus gem/cis, only 58-68% of patients received chemotherapy as planned. Radical cystectomy was performed in 91% of patients, meaning that 9% of patients did not receive previously planned cystectomy.4
 Furthermore, AEs are not insignificant with these NAC regimens as demonstrated in the table below:
Furthermore, AEs are not insignificant with these NAC regimens as demonstrated in the table below: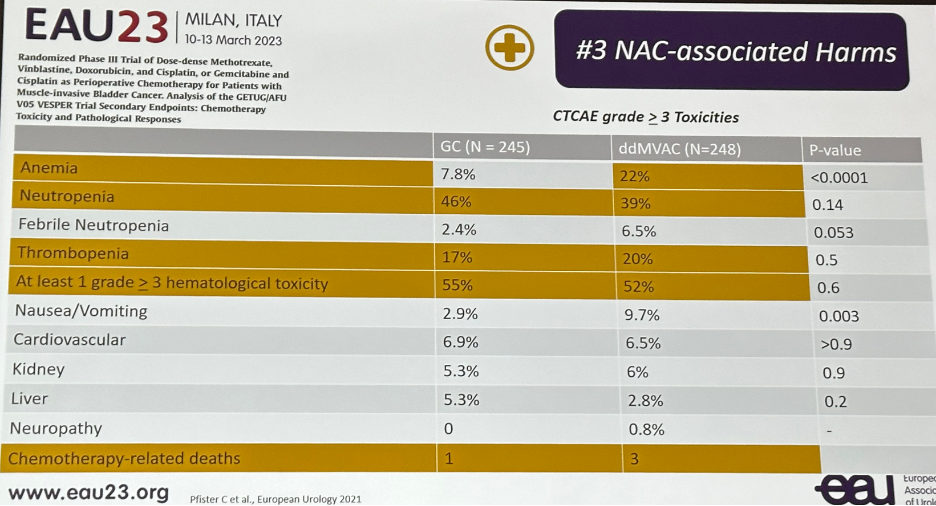 Other notable complications include the development of sarcopenia, which has been evaluated by Dr. Psutka’s group. Up to 69% of such patients become sarcopenic during follow-up with a % change in skeletal muscle index of -6.4%.
Other notable complications include the development of sarcopenia, which has been evaluated by Dr. Psutka’s group. Up to 69% of such patients become sarcopenic during follow-up with a % change in skeletal muscle index of -6.4%.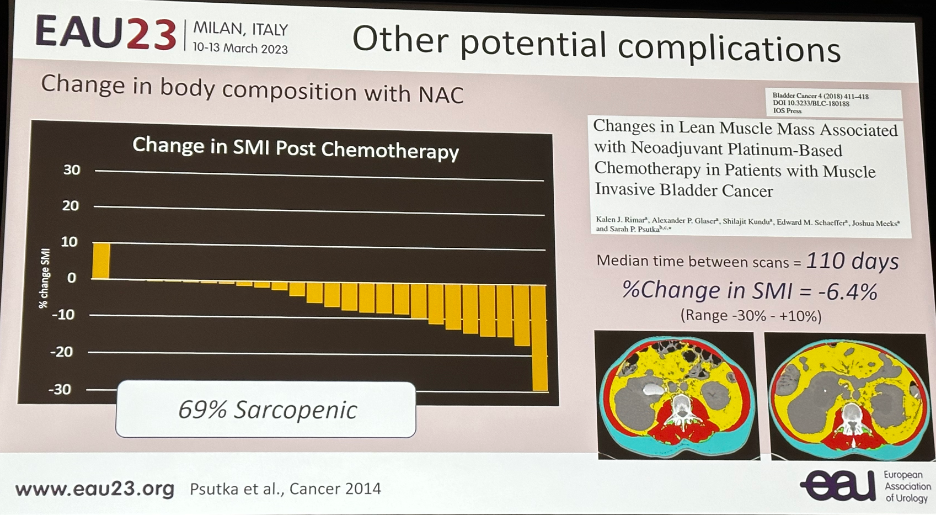 Furthermore, after NAC we note statistically significant declines in:
Furthermore, after NAC we note statistically significant declines in:- Physical well-being
- Functional well-being
- GI symptoms: weight loss, diarrhea, appetite
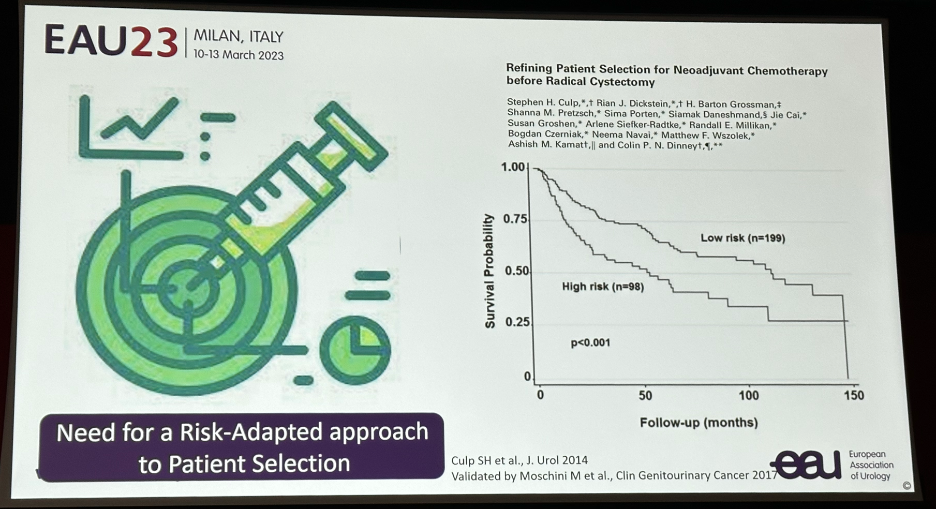
 Another important issue is that we are still unable to reliably predict which patients may potentially benefit most from NAC, and thus adopt a risk-adapted approach to patient selection. The MDACC high risk criteria may help identify patients most likely to benefit from NAC using clinical/pathologic criteria:
Another important issue is that we are still unable to reliably predict which patients may potentially benefit most from NAC, and thus adopt a risk-adapted approach to patient selection. The MDACC high risk criteria may help identify patients most likely to benefit from NAC using clinical/pathologic criteria:- Hydroureteronephrosis
- cT3b-4a disease (palpable 3-D mass on EUA, prostate stromal invasion)
- Lymphovascular invasion
- Variant histology
 There is significant research in this field with novel data emerging that BASQ-like tumors are more likely to achieve a pathologic complete response (FOXA1/GATA3 low; KRT5/6/15 high). Additionally, the Immunoscore (CD3+/8+ T-Cell density) is another biomarker that has been shown to be associated with pathologic complete responses.
There is significant research in this field with novel data emerging that BASQ-like tumors are more likely to achieve a pathologic complete response (FOXA1/GATA3 low; KRT5/6/15 high). Additionally, the Immunoscore (CD3+/8+ T-Cell density) is another biomarker that has been shown to be associated with pathologic complete responses. 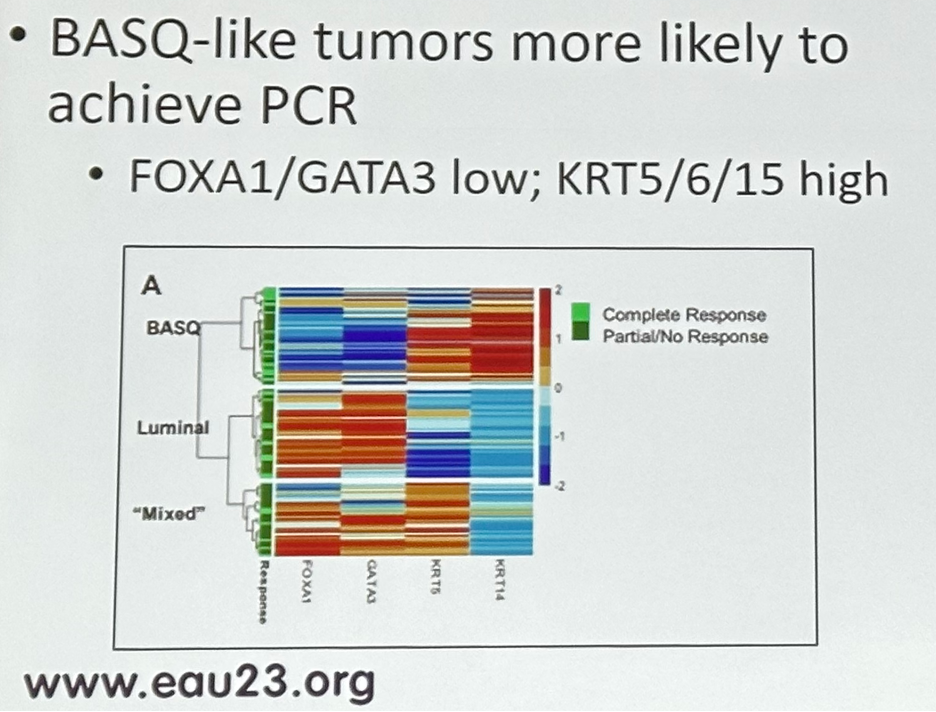 Research into IHC predictors of pathologic complete response are currently ongoing to help select patients that are most likely to benefit from NAC.
Research into IHC predictors of pathologic complete response are currently ongoing to help select patients that are most likely to benefit from NAC.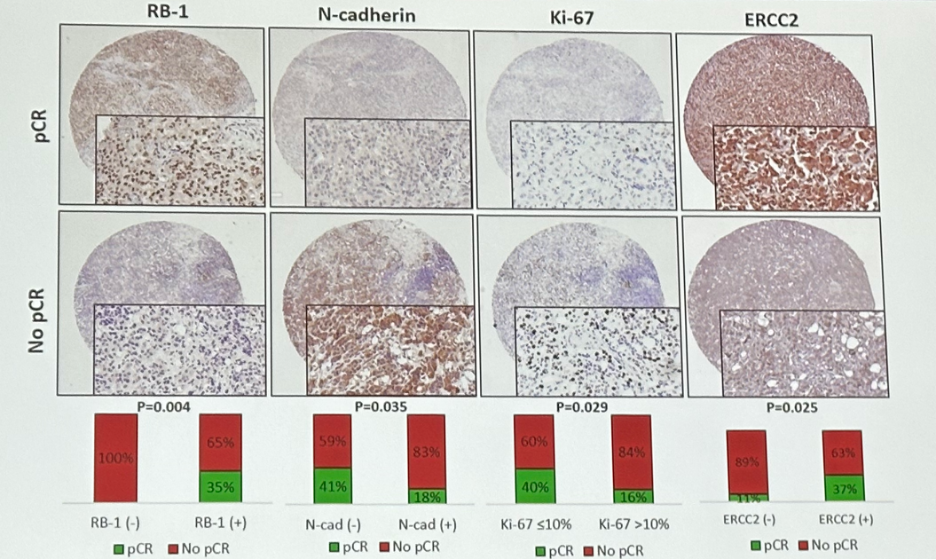 Going back to the case presented by Dr. Baboudjian, Dr. Psutka asked the question: “If she had gone straight to surgery…could she have had a better outcome?” The patient experienced grade 4 thrombocytopenia with 6 cycles of ddMVAC that could have been avoided and likely delayed surgery. Furthermore, she had ypT2bN1R0 on the RC specimen, which suggests a lack of a pathologic response to chemotherapy that puts her at higher risk of clinical progression. Furthermore, the patient developed cisplatin-related toxicity, which required subsequent use of carboplatin, which is likely to be associated with inferior long-term outcomes. As such, Dr. Psutka concluded that this patient would have likely benefited from NAC avoidance prior to RP.
Going back to the case presented by Dr. Baboudjian, Dr. Psutka asked the question: “If she had gone straight to surgery…could she have had a better outcome?” The patient experienced grade 4 thrombocytopenia with 6 cycles of ddMVAC that could have been avoided and likely delayed surgery. Furthermore, she had ypT2bN1R0 on the RC specimen, which suggests a lack of a pathologic response to chemotherapy that puts her at higher risk of clinical progression. Furthermore, the patient developed cisplatin-related toxicity, which required subsequent use of carboplatin, which is likely to be associated with inferior long-term outcomes. As such, Dr. Psutka concluded that this patient would have likely benefited from NAC avoidance prior to RP.Presented by: Dr. Sarah Psutka, MD, MSc, Associate Professor, Department of Urology, University of Washington, Seattle, WA
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Association of Urology (EAU) Annual Meeting, Milan, IT, Fri, Mar 10 – Mon, Mar 13, 2023.
References:
- Grossman, et al. Neoadjuvant Chemotherapy plus Cystectomy Compared with Cystectomy Alone for Locally Advanced Bladder Cancer. N Engl J Med, 2003. 349:859-866
- Bajorin, et al. Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. N Engl J Med, 2021. 384:2102-2114.
- Galsky, et al. A consensus definition of patients with metastatic urothelial carcinoma who are unfit for cisplatin-based chemotherapy.Lancet Oncol, 2011.(3):211-214.
- Pfister, et al. Dose-Dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin or Gemcitabine and Cisplatin as Perioperative Chemotherapy for Patients With Nonmetastatic Muscle-Invasive Bladder Cancer: Results of the GETUG-AFU V05 VESPER Trial. J Clin Oncol, 2022. (18):2013-2022.