(UroToday.com) At the European Association of Urology (EAU) Virtual 2020 meeting’s Immunotherapy and Beyond Thematic session, Dr. Joost Boormans discussed PD-1/PD-L1 inhibitors replacing perioperative chemotherapy for urothelial cancer.
Dr. Boormans notes that there is level 1 evidence in favor of cisplatin-based chemotherapy in patients with cT2-cT4aN0-1M0 muscle invasive bladder cancer. In a nationwide population-based study, Hermans et al.1 showed that among 10,338 patients with cTa/is,T1-4,N0-N3,M0-1 patients in the Netherlands, 86% did not receive peri-operative treatment, 7.0% received neoadjuvant chemotherapy, 3.2% neoadjuvant radiotherapy, 1.8% adjuvant chemotherapy, and 2.1% adjuvant radiotherapy. However, neoadjuvant chemotherapy use increased from 0.6% in 1995 to 21% in 2013 (p < 0.001), and use of neoadjuvant radiotherapy decreased from 15% to 0.4% (p < 0.001). Furthermore, comparable temporal trends were found in 6,032 patients staged cT2-4N0M0.
Dr. Boormans notes that in clinical trials, downstaging to ypT0N0 occurs in 30-40% of patients, but in general clinical practice, ypT0N0 rates are only 25%. We know that those with clinical downstaging to ypT0N0 ultimately do quite well with 5-year OS rates of ~80%. However, many patients are non-responders to chemotherapy, which may delay curative surgery, lead to toxicity (35% Grade III/IV complications), and lead to higher rates of pN+/M+ disease. Indeed, controversies in neoadjuvant chemotherapy remain. Pro’s for neoadjuvant chemotherapy include (i) this is the earliest stage of the disease, (ii) the patient’s condition is good, (iii) there is the opportunity for pathological downstaging, (iv) eradication of micromets, and (v) a proven survival benefit. Cons of neoadjuvant chemotherapy include (i) overtreatment of low-risk disease, (ii) toxicity and cost, (iii) delay of cystectomy, (iv) 35% of patients have renal insufficiency, and (v) many patients have comorbidities (cardiac, hearing disorders, peripheral arterial occlusive disease). According to Dr. Boormans, there is room for improvement for neoadjuvant therapy for patients with muscle-invasive bladder cancer. Dr. Boormans notes that there is no level 1 evidence in favor of adjuvant chemotherapy, and studies have been hampered by poor accrual of patients. Perhaps, there is difficulty in motivating both patients and physicians to enroll in these studies.
Perioperative checkpoint inhibitors have become more impactful over the last several years. PD-(L)1 is expressed in urothelial carcinoma, which has a high mutational load. Treatment with PD-(L)1 inhibitor has previously shown a survival benefit in patients with advanced urothelial carcinoma, is feasible in cisplatin-unfit advanced urothelial carcinoma patients and is better tolerated than chemotherapy in patients with metastatic urothelial carcinoma. The following figure excellently demonstrates the comparison between the neoadjuvant immunotherapy trials ABACUS, A phase II study investigating the safety and efficacy of neoadjuvant atezolizumab in muscle-invasive bladder cancer (ABACUS) and PURE-01, Neoadjuvant Pembrolizumab for Muscle-invasive Urothelial Bladder Carcinoma (PURE-01):

For both of these studies, much attention has been given to predictive biomarkers for immunotherapy response. In ABACUS, PDL1 expression, tumor mutation burden and DDR gene mutations did not correlate with pathologic complete response, which contradicts the predictive ability of these biomarkers in the metastatic setting. Additionally, higher levels of CD8+ T-cells were seen in responders, and the 8-gene T-cell signature was associated with response. In the PURE-01 trial, mean PDL1 expression and mean tumor mutational burden were associated with pathologic complete response. However, DDR gene mutations, FGFR3 mutations, and variant histology were not associated with pathologic complete response. Looking at the safety profile, pembrolizumab (PURE-01) was generally better tolerated than atezolizumab (ABACUS).
The phase 2 NABUCCO trial was a single-arm study of 24 patients that were treated with three cycles of neoadjuvant combination ipilimumab plus nivolumab, initially presented at ESMO 2019: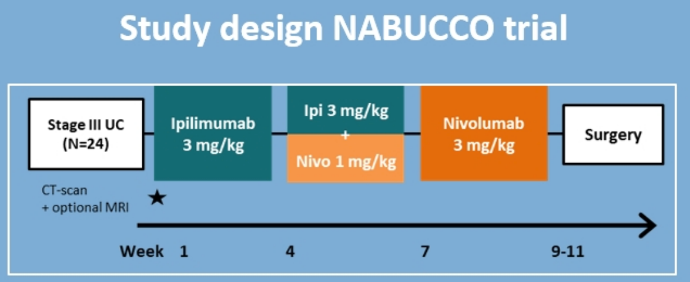
The primary endpoint was time to radical cystectomy <12 weeks and the secondary endpoint was pathologic complete response. Importantly, 23 of 24 patients had resection <12 weeks after treatment and only six patients received <3 cycles of treatment. Pathologic complete response was achieved in 11 of 24 patients (46%). With regards to safety, 55% of the total population had grade 3-4 immune-related adverse events, which was decreased to 41% when excluding clinically insignificant lipase elevations. The 30-day mortality rate after surgery was 0%, and 90-day mortality rate was 4%.
This is a disease-space that is burgeoning with ongoing trials, including 24 ongoing phase I/II trials looking at neoadjuvant immunotherapy +/- neoadjuvant chemotherapy. Furthermore, there are several key phase III trials of neoadjuvant therapy plus radical cystectomy: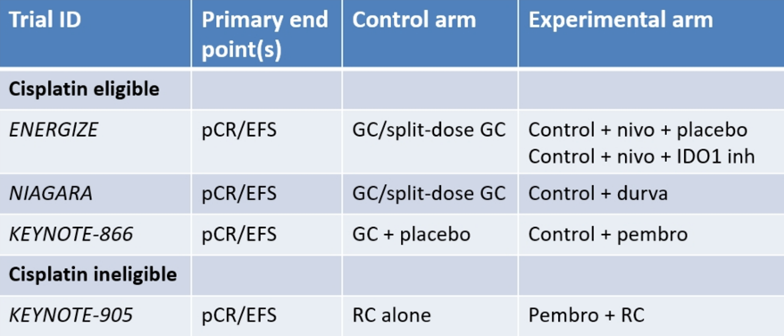
As was previously presented at ASCO 2020, unfortunately, the IMvigor 010 study assessing atezolizumab vs observation (no placebo) following radical cystectomy was a negative study. In IMvigor 010, 809 patients stage with ypT2-4aN0 or ypN positive (surgical margin negative) or stage pT3/4 or pN positive (surgical margin negative) patients were randomized and did not meet the primary endpoint of disease-free survival.
Some final considerations were also provided by Dr. Boormans:
- There are no randomized phase III data reported as of yet
- Not all trials are placebo-controlled
- There is selection towards low-stage and low-volume disease
- The efficacy of immunotherapy monotherapy in advanced urothelial carcinoma is questionable
- The combination of ipilimumab plus nivolumab seems promising in locally advanced muscle invasive bladder cancer
- Predictive biomarkers for neoadjuvant therapy seem to differ than from those in the M+ setting
Dr. Boormans concluded his presentation with the following take-home messages:
- Neoadjuvant treatment with immunotherapy is feasible in muscle-invasive bladder cancer patients undergoing radical cystectomy
- The toxicity profile of immunotherapy seems favorable compared to neoadjuvant chemotherapy
- In early studies, the delay in time to surgery is limited
- Postoperative complications are not higher than for those undergoing neoadjuvant chemotherapy
- Complete pathological response rates are similar compared to those receiving neoadjuvant chemotherapy
Finally, some future perspectives from Dr. Boormans:
- Will immunotherapy replace chemotherapy in the neoadjuvant setting? Yes, in the cisplatin-ineligible population
- Will immunotherapy be added to chemotherapy in the neoadjuvant setting? Probably in the cisplatin eligible population
- Will immunotherapy combination therapy outperform chemotherapy? This is still open for debate, particularly in the locally advanced/induction setting
Presented by: Joost L. Boormans, MD, Ph.D., Erasmus MC Cancer Institute, Rotterdam, The Netherlands
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the Virtual 2020 EAU Annual Meeting #EAU20, July 17-19, 2020
References
1. Hermans TJ, van de Putte EEF, Horenblas S, et al. Perioperative treatment and radical cystectomy for bladder—A population based trend analysis of 10,338 patients in the Netherlands. Eur J Cancer 2016 Feb;54:18-26.
Related Content:
Watch: IMvigor010 Primary Analysis from a Phase III Randomized Study of Adjuvant Atezolizumab versus Observation in High-Risk Muscle-Invasive Urothelial Carcinoma - Thomas Powles & Matthew Galsky
Read: AUA 2020: Association of Pathologic Response to Neoadjuvant Pembrolizumab with Tumor Subtype from the PURE-01 Study