(UroToday.com) As part of the “Game-changing Session 2” plenary presentation at the European Association of Urology (EAU) Virtual Annual Meeting, Dr. Oliver Grimm presented an analysis of the recurrence risk in patients with High Grade Non-Muscle Invasive Bladder Carcinoma in the Randomised Phase III Clinical Trial ‘NIMBUS’ stratified for European Organization for Research and Treatment of Cancer (EORTC) and Spanish Urology Association for Oncological Treatment (CUETO) risk categories.
For patients with intermediate or high-risk NMIBC and those with carcinoma in situ (CIS), adjuvant treatment with bacillus calmette-guerin (BCG) is guideline-recommended on the basis of proven benefits in disease recurrence. The recommended dosing approach involves 6 weekly induction doses following by 3 weekly maintenance doses at 3, 6, and 12 months. While efficacious, BCG instillation is associated with frequent adverse events which may lead to discontinuation. As a result, a number of studies (including EORTC 30962 and CUETO 98013) have sought to assess changes to treatment which may reduce symptom burden. The NIMBUS trial investigated whether a reduced frequency of BCG instillation during the induction and maintenance phases would result in similar clinical efficacy to standard BCG treatment protocols with lower adverse events, inconvenience, and cost.
As highlighted in the flow diagram below, the investigators enrolled patients with BCG-naïve high grade non-muscle invasive bladder cancer. This could be primary or recurrent disease, solitary or multiple tumors, with or without concurrent CIS, and with the absence of high-grade papillary disease following repeat transurethral resection of bladder tumor (TURBT)
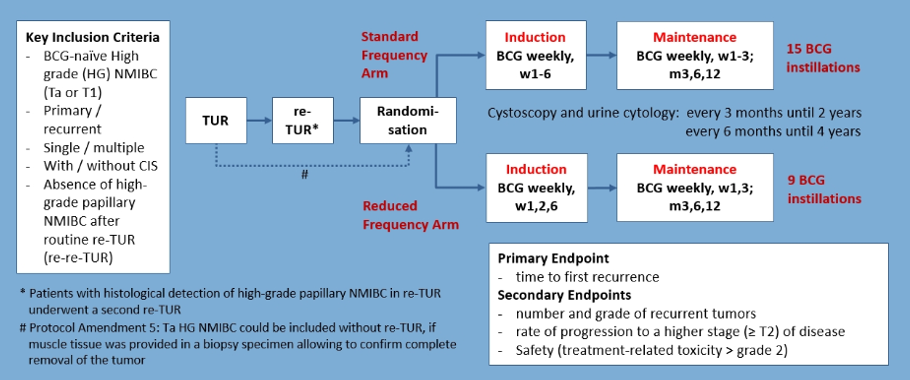
Patients were then randomized to the standard BCG protocol with 6 weekly induction treatments followed by 3 weekly maintenance treatments at 3, 6, and 12 months. In the intervention arm, patients received BCG at 1, 2, and 6 weeks followed by maintenance at weeks 1 and 3 at 3, 6, and 12 months. As a result, over 12 months, patients in the standard arm received 15 BCG instillations while those in the reduced frequency arm received 9 BCG instillations.
The primary outcome of interest was the time to the first recurrence while key secondary outcomes included the number and grade of recurrent tumors, the rate of progression to muscle-invasive disease, and safety (including treatment-related adverse events > grade 2).
The authors powered this study on the basis of therapeutic equivalence defined as the lower bound of the 95% confidence interval being higher than the hazard ratio of 0.75 for recurrence. This resulted in a sample size of 1000 total patients to give a power of 80%. Recruitment was delayed on account of BCG shortage which modified statistical assumptions. As a result, a total of 824 patients were then targeted.
However, at the time of data cut-off (July 1, 2019), the authors report on data from 345 randomized patients.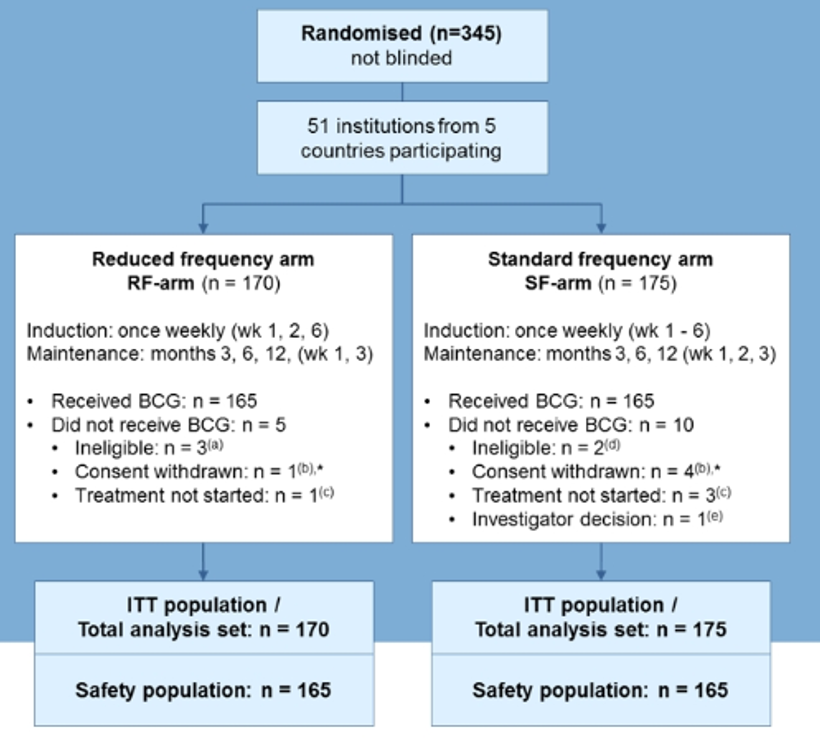
Baseline characteristics were well balanced between the two groups, including center of randomization, Ta vs T1 disease, concomitant CIS, single vs multiple tumors, and BCG strain (Medac, Connaught, or Tice).
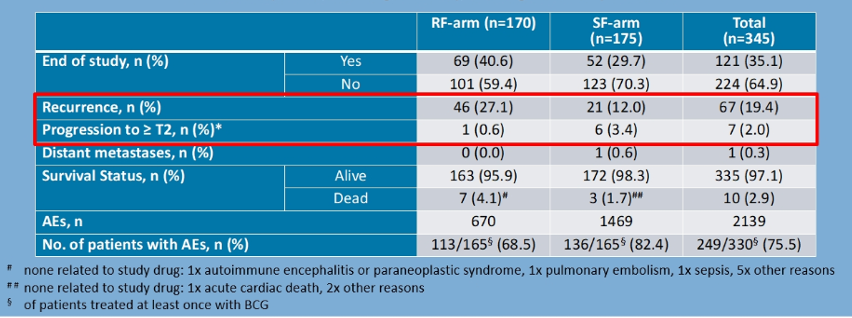
In the overall population, 67 patients (19.4%) of patients had recurrence and 7 (2%) had progression to muscle-invasive disease. Rates of recurrence were somewhat higher in patients in the reduced frequency arm (27% vs 12%) while progression was somewhat lower in these patients (0.6% vs 3.4%).
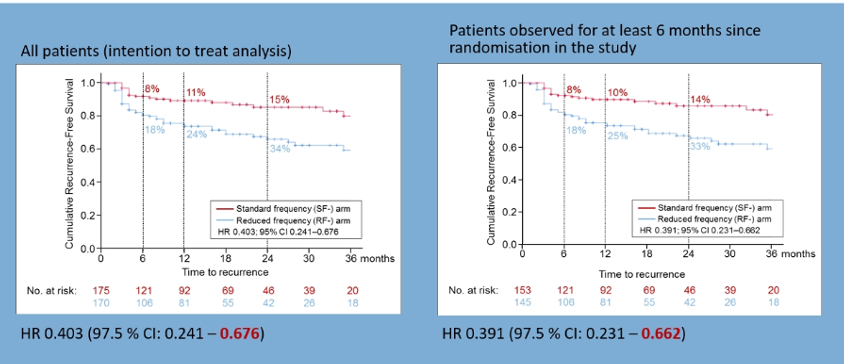
Assessing time to recurrence utilizing the Kaplan Meier method, the authors found a significantly lower recurrence-free survival among patients who received the reduced frequency of BCG.
In the NIMBUS cohort, rates of recurrence were lower than predicted based on the EORTC probability of recurrence. Similarly, among patients with CUETO scores of 5-6 or 7-9, rates of recurrence in the NIMBUS cohort were lower than predicted. Dr. Grimm suggested that this was due to the routine use of repeat TURBT in this study cohort.

Presented by: Professor Marc-Oliver Grimm, MD, Director of Klinik für Urologie, Universitätsklinikum Jena, Germany
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, @WallisCJD on Twitter at the 35th Annual EAU Congress, 2020 Virtual Program #EAU20, July 17-19, 2020.
Related Content:
Read: ASCO GU 2020: Treatment of High-Grade Non-Muscle Invasive Bladder Carcinoma: Results of the Phase III Clinical Trial (NIMBUS)