The authors of this abstract describe their experience with PRX302, a genetically modified pore-forming protein (aerolysin) activated intraprostatically only by enzymatically active PSA – thereby limiting activity to the prostate alone. This abstract describes their Phase II trial results – as such, the focus was toxicity, side effects and potential efficacy.
Eighteen patients with clinically significant localized cancer defined as either Gleason ≤ 4+3 with a maximum cancer core length (MCCL) ≤ 10mm, or Gleason 3+3 with MCCL ≥ 4mm. All patients had a single pre-identified lesion injected transperineally using MRI-ultrasound elastic image-fusion software (SmartTarget®), under general anaesthetic, with up to 5mL of a standard dosing solution of 20ug/mL PRX302. Follow-up occurred at 2 days (teleconsult) and at 2, 6, 12, 24 and 26 weeks. A mpMRI-targeted transperineal biopsy of the treated area was carried out at 24 weeks (6 months).
Median age and PSA were 66.50 years (IQR 13.00) and 6.25ng/ml (IQR 2.45), consistent with localized disease. Of the eighteen patients, 14 (78%) had Gleason 7 cancer with median lesion size of 0.3 cm (IQR 0.2-0.5), so all the lesions were quite small. No patients were lost to follow-up; all patients completed the study.
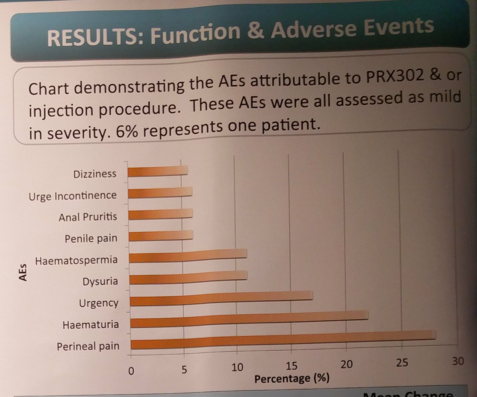
No serious adverse events were noted through the study. Summary of complications:
In terms of efficacy and oncologic outcome, the follow-up was short. Biopsy data at 24 weeks following treatment showed that only 2 men (11%) had complete tumour ablation with no histological evidence of any cancer at 6 months. Seven (39%) had partial ablation defined as reductions in MCCL or Gleason grade; 9 men (50%) had no histological response and in some cases experienced an increase in MCCL or upgrading. Urinary and sexual function was preserved.
From an outcomes standpoint, I find these results to be underwhelming. While safe for the patient, a 50% insufficient treatment rate (with 39% having reduction but not resolution) is concerning. The authors felt the same way, and are considering dose adjustment and optimizing tumor delivery (as tissue saturation is required, they are considering continuous slow infusion).
Speaker: Y. Shanmugabavan
Co-Author(s): Bass E., Hulme A., Freeman A., Brew-Graves C., Potyka I., Ramachandran N., Emberton M., Ahmed H.U.
Institution(s):
1. University College London, Division of Surgery and Interventional Sciences, London, United Kingdom
2. Sophiris, Sophiris Bio Corporation, California, United States of America
3. University College London Hospital, Dept. of Histopathology, London, United Kingdom
4. University College London Hospital, Dept. of Radiology, London, United Kingdom
Written By: Thenappan Chandrasekar, MD, Clinical Fellow, University of Toronto
Twitter: @tchandra_uromd
at the #EAU17 - March 24-28, 2017- London, England