- In non-metastatic CRPC setting after apalutamide or enzalutamide – we can either give abiraterone1 or docetaxel2.
- In denovo metastatic disease after abiraterone – we can give either enzalutamide3 or docetaxel4
- In denovo metastatic disease after docetaxel – we can give docetaxel re-challenge5, abiraterone or enzalutamide6, PARP inhibitor7, or Radium 2238
A retrospective analysis demonstrated the response rates of patients receiving initial treatment with hormonal therapy, docetaxel and cabazitaxel, and secondary hormonal treatment.9 The data demonstrated that rapid progression to CRPC (<12 months) was associated with a low response to secondary hormonal therapy. Additionally, PSA response to taxanes did not seem to be affected by the time for CRPC to develop.
Another study demonstrated a prognostic model for predicting response to abiraterone and overall survival in mCRPC patients. This proposed prognostic model identified six predictive factors:
- LDH> upper normal limit
- ECOG status 2 compared to 0-1
- Liver metastases present
- Albumin (<=4 g/dl vs. > 4 g/dl)
- Alkaline phosphatase > upper normal limit
- The time frame between starting androgen deprivation therapy (ADT) until the initiation of abiraterone is <=36 months compared to >36 months.
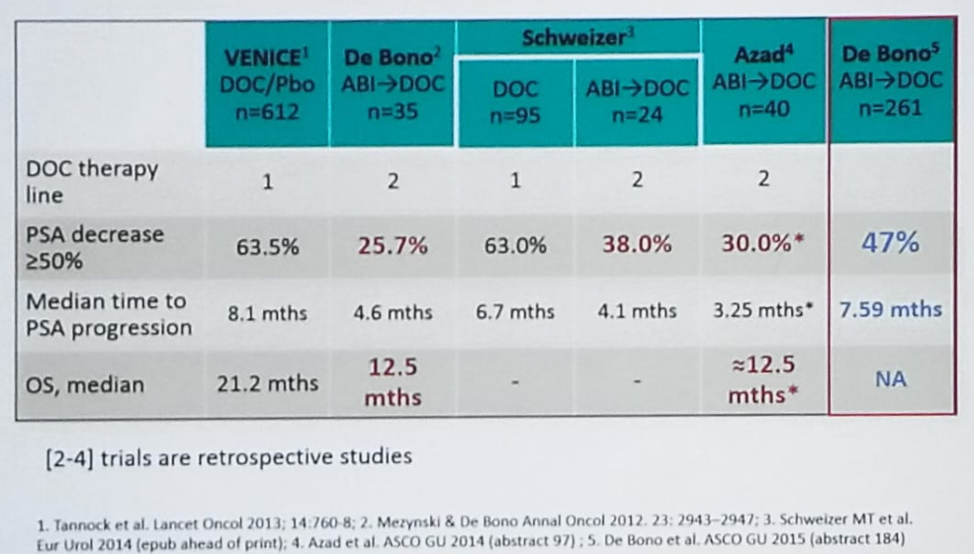
Figure 1 – Does Abiraterone Before Docetaxel Decrease Efficacy of Taxanes in mCRPC Patients?
In the ASCO meeting in 2017, a randomized phase 2 cross-over study of abiraterone + prednisone vs. enzalutamide for patients with mCRPC16 was presented (study schema is shown in figure 2). In this study mCRPC treatment naïve patients were randomized to either abiraterone or enzalutamide, and when progression was evident, they were switched to the other treatment. This study demonstrated that enzalutamide initially had better PSA response rates than abiraterone initially. However, no difference was discerned in the time to PSA progression between both groups. The authors also demonstrated that the detection of circulating tumor DNA was associated with measures of tumor burden and poor outcomes. Lastly, genomic alterations in BRCA2/ATM, TP53, PI3K pathway, RB1, and AR were associated with earlier progression and primary resistance.
Figure 2 – Study Schema of the Randomized Phase 2 Cross-over Study of Abiraterone + Prednisone vs. Enzalutamide for Patients with mCRPC

When assessing the results of the crossover in this study, PSA response rate and time to progression were better for 2nd line enzalutamide compared to 2nd line abiraterone. The sequence of abiraterone + prednisone followed by enzalutamide was associated with a trend toward a longer time to 2nd progression, and again, the presence of circulating tumor DNA was associated with worse outcomes.
Dr. Hotte concluded his talk and summarized that there are currently multiple choices of treatment with little level one evidence to help with deciding which treatment sequence to use. Most probably, it is more prudent to start with abiraterone, if possible. In a patient with poor prognosis, starting therapy with taxanes should be considered. Most importantly, the multidisciplinary approach must be utilized with these patients for optimal treatment and outcomes. Lastly, these men still die due to mCRPC, and continuing to enroll in clinical trials is extremely important.
Presented by: Sebastien Hotte, MD, MSc (HRM), FRCPC, Lead and Co-Principal Investigator, McMaster Translational Research Team, Associate Professor, Department of Oncology, Division of Medical Oncology
McMaster University
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter: @GoldbergHanan at the CUOS – Canadian Uro-Oncology Summit 2019, #CUOS19 January 10-12, 2019 Westin Harbour Castle, Toronto, Ontario, Canada
References:
1. Noonan et al. Ann Oncol 2013
2. De Bono et al. Eur Urol 2017
3. De Bono et al. Eur Urol 2018
4. De Bono et al. Eur Urol 2017
5. Lavaud et al. Eur Urol 2018
6. Scher HI. Et al. NEJM 2012
7. Clarke et al. Lancet Oncol 2018
8. Sartor et al. Prostate 2016
9. Angelegus A et al. JCO 2014
10. Loriot Y et al. Ann Oncol 2013
11. Noonan KI et al. Ann Oncol 2013
12. Schrader A et al. Eur Urol 2014
13. Bianchini D et al. Eur J cancer 2014
14. Thomsen FB et al. Scand J Urol Nephrol 2014
15. Badrising S et al. Cancer 2014
16. Kim N et al. ASCO 2017