Dr. Trinh began by highlighting the massive effect of the COVID-19 pandemic on society at large, on medicine, and on the health care system as a whole. While there was initially a large focus on patients who have been infected and hospitalized with COVID-19, over time it has become more apparent that the effects of this pandemic have stretched to include many patients who were never infected but had their care for other conditions affected. The first widespread awareness of the greater health systems implications of COVID-19 came from the cancelation of surgeries. While this was documented academically by the CovidSurg group, lay-press headlines and anecdotal cases did more to drive public awareness.
The rationale for postponing scheduled procedures in light of the COVID-19 pandemic is multi-faceted: to preserve resources (including ventilators and personal protective equipment) for an expected surge of cases, to mitigate infectious risks to our patients undergoing elective surgery, and to mitigate risks to the surgical and anesthesia teams.
To contextualize the effects of COVID-19 on genitourinary cancer care, Dr. Trinh highlighted the continuum of risk and complexity in care ranging from office visits and routine laboratory investigators to major surgical procedures.
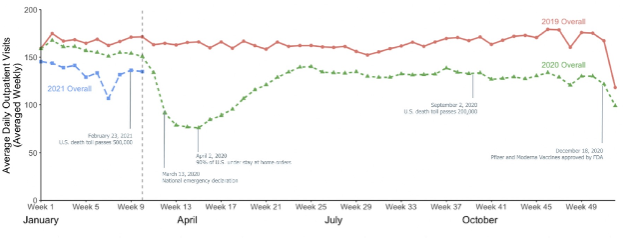
Using their health systems data, Dr. Trinh and colleagues assessed the effect of COVID-19 and the related changes in health care delivery on cancer screening tests and subsequent cancer diagnosis, including mammography for breast cancer, PSA testing for prostate cancer, colonoscopy for colon cancer, Papanicolaou tests for cervical cancer, and low-dose CT scans for lung cancer. Each of these declined significantly compared both with the immediately preceding 3 months and the same time frame the year prior (2019). However, in the same health system, they subsequently showed in a follow-up paper that there was a recovery of cancer screening. However, this recovery was not equal across socioeconomic, racial, and ethnic groups. Thus, the pandemic has the potential to exacerbate existing health disparities.
Moving from single system data to more broad datasets, Dr. Trinh then highlighted work led by Dr. Cooperberg using the AQUA registry which documented a similarly large decrease in urologic cancer care during the pandemic. In this context, however, there has not been a return to baseline levels.
While delays in treatment have proven inevitable in the context of the pandemic, Dr. Trinh highlighted a number of studies including a European Urology collaborative review across genitourinary cancers, a systematic review focusing on patients with intermediate and high-risk prostate cancer, and an assessment of a variety of common cancers to examine whether treatment delays are safe and if so, for which patients. In general, this is a context-dependent answer with both patients and clinicians needing to weigh the oncologic risks of delayed cancer care (were present) with the risks of COVID-19 to the patient, the treating health care professionals, and the health care system.
He then discussed the clinical guidelines adopted at Dana Farber and Brigham and Women’s Cancer Center. These include deferring care for all patients with low-risk prostate cancer and most with favorable intermediate-risk disease. For those with intermediate-risk disease, neoadjuvant ADT was not recommended while for those with high- and very high-risk disease, a consideration for neoadjuvant and adjuvant ADT with or without apalutamide (in keeping with the PROTEUS protocol) could be considered.
Dr. Trinh then highlighted work considering the effects of these delays on cancer surgery on the patient experience. Initial patient responses were typically negative (and associated with worry and lack of control) though some patients suggested that they expected it or were relieved. Communication between the patient and physician was critical in addressing concerns.
Finally, Dr. Trinh emphasized that this pandemic may exacerbate racial disparities, in particular noting that there was a significant decrease in mammography testing among Black and Hispanic women. However, no such effect was observed for PSA testing.
Presented by: Quoc-Dien Trinh, MD, Associate Professor of Surgery at Harvard Medical School, Co-Director of the Dana-Farber/Brigham and Women's Prostate Cancer in Boston, Mass
Written by: Christopher J.D. Wallis, University of Toronto Twitter: @WallisCJD during the 2021 American Urological Association, (AUA) Annual Meeting, Fri, Sep 10, 2021 – Mon, Sep 13, 2021.