Observational studies have suggested such benefit may also be seen with radical prostatectomy2 but this has not previously been examined in a RCT. Dr. Sooriakumaran reported on the world’s first RCT, TRoMbone, on the safety and feasibility of randomization to systemic therapy plus radical prostatectomy in synchronous oligo-metastatic prostate cancer.
The initial TRoMbone protocol randomized men with synchronous oligo-metastatic prostate cancer (1-3 skeletal metastases on conventional imaging) who were < 75 years old and ECOG PS 0-1, to radical prostatectomy and extended pelvic lymphadenectomy within 3 months of starting standard care systemic therapy versus standard care systemic therapy alone. Importantly, with the recent uptake of chemotherapy in hormone naïve men, the protocol was amended to allow patients to have docetaxel prior to radical prostatectomy, and to increase the number of recruitment sites from 3 to 9.
Among the 176 patients screened, 71 were eligible; of those, 51 (71.8%) were randomized including 24 to radical prostatectomy. High recruitment rates were achieved with use of a quintet recruitment investigation. This identified the commonest causes of non-recruitment as: patients not wanting surgery; lack of clinician equipoise; and, (before the protocol amendment) inability to have docetaxel preoperatively. As a result of the protocol amendment, recruitment completed four months ahead of schedule with 7/9 (77.8%) sites successfully recruiting at least one patient. So far, there have been eight surgeons that have performed a radical prostatectomy. Thus far, roughly half of the surgical patients have received docetaxel preoperatively, and all had received ADT.
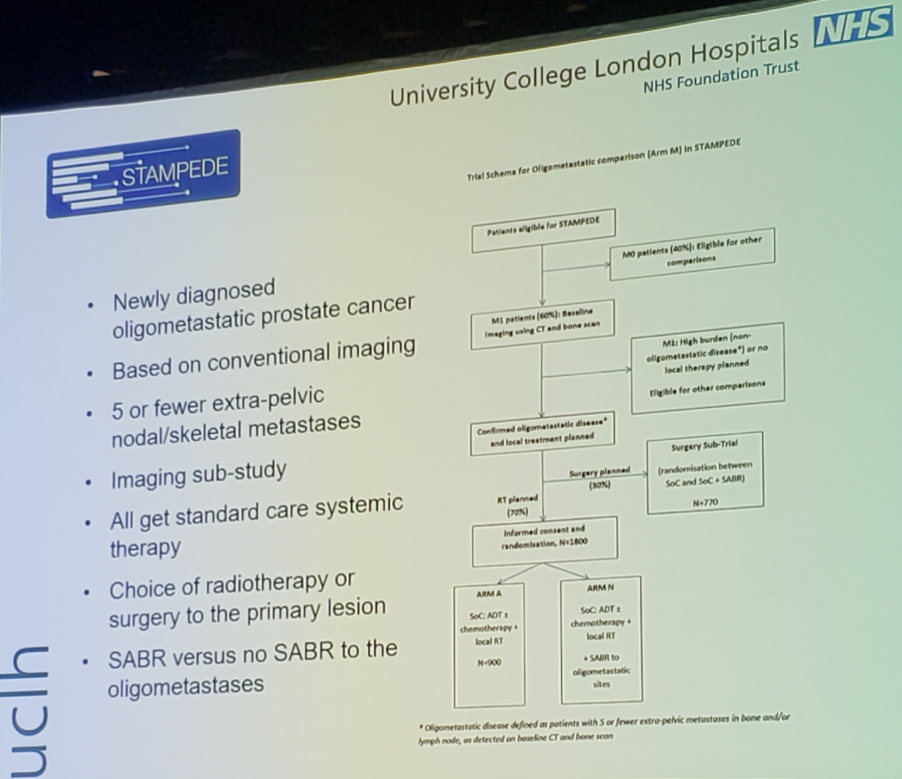
Impressively, 100% of radical prostatectomies have been conducted with robotic assistance, no cases were abandoned, and the only complication to date is a rectal injury (repaired intraoperatively with primary closure; that same patient was the only one who required a blood transfusion). Surgical challenges have included (i) posterior dissection avoiding a rectal injury, (ii) more difficult endopelvic fascia dissection, and (iii) a more difficult pelvic lymph node dissection. Quality-of-life data demonstrated equivalence in EQ5D scores between the Control and Intervention groups, and satisfaction scores were high even in those who received ADT, docetaxel, and radical prostatectomy. Thus far, the positive surgical margin rate is 43%, higher than the literature standard of ~15-20% based on the high-risk nature of the operation, and 78% of patients have had pT3b disease. Secondary to the feasibility of enrollment into TRoMbone, pending funding, STAMPEDE will open Arm M, a surgical arm for patients with oligometastatic disease:
Dr. Sooriakumaran concluded his presentation with several key points:
- TRoMbone has demonstrated that it is feasible to randomize UK men with synchronous oligo-metastatic prostate cancer to standard care systemic therapy versus that plus locally-directed surgery
- Robotic prostatectomy in oligometastatic disease is technically feasible
- Early results demonstrate acceptable peri-operative and short-term oncological outcomes
- Interim outcomes suggest the procedure is safe and technically feasible, and a full RCT is being planned
Co-Authors: Prabhakar Rajan, Omar Al Kadhi, John Kelly, London, United Kingdom, Jonathan Aning, Naeem Soomro, Newcastle, United Kingdom, Richard Bryant, Alastair Lamb, Oxford, United Kingdom, Paul Cathcart, Oussama Elhage, London, United Kingdom, Christopher Eden, Guildford, United Kingdom, Imran Ahmad, Hing Leung, Glasgow, United Kingdom, Senthil Nathan, London, United Kingdom, Freddie Hamdy, Oxford, United Kingdom
Written By: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University - Medical College of Georgia @zklaassen_md at the American Urological Association's 2019 Annual Meeting (AUA 2019), May 3 – 6, 2019 in Chicago, Illinois
References:
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet 2018 Dec 1;392(10162):2353-2366.
- Leyh-Bannurah SR, Gazdovich S, Budaus L, et al. Local therapy improves survival in metastatic prostate cancer. Eur Urol 2017 Jul;72(1):118-124.