Patients’ CT images were converted to virtual reality models (Figure 1), which surgeons and patients viewed on an Oculus Rift virtual reality headset prior to the PCNL. Preoperatively, surgeons recorded whether the model was helpful in preoperative planning (e.g. for choosing the appropriate calyx to enter), and patients recorded whether viewing the models improved their understanding of where the stone was located and if viewing the model lessened their preoperative anxiety about the procedure.
Indeed, both surgeons and patients found the virtual reality models helpful. For surgeons, the models enhanced their understanding of the patient’s anatomy and the optimal calyx of entry. In fact, after viewing the virtual reality models, surgeons changed their operative approach in 40% of cases. For patients, the models resulted in an improvement in the understanding of the location of their stone and also quelled their preoperative anxiety. Regarding operative outcomes compared to a retrospectively matched cohort, there was a significant decrease in fluoroscopy time and estimated blood loss in the virtual reality group (Table 1).
The presenter was questioned about the retrospective nature of the matched-pair analysis, which he acknowledged was a limitation of the study. He did indicate that his group is currently performing a prospective randomized trial in order to assess the true effect of virtual reality for preoperative planning on operative outcomes.

Figure 1: Virtual Reality Model.
A)Transparent view of kidney and surrounding anatomy. Lower pole and interpolar renal calculi in yellow are highlighted by solid red arrows. B)Posterior view of pertinent anatomy; planned nephrostomy tract is above the 12th rib (green solid arrow).
C)Intrarenal view as the iVR user proceeds above the 12th rib and “looks” into the planned upper pole calyceal point of entry (yellow solid arrow).
D)View as the iVR user travels further through the upper pole calyx and along the upper pole infundibulum. The user visualizes the upper border of the yellow stone (thick red arrow) and can see how the stone branches into the lower pole (thin red arrow)
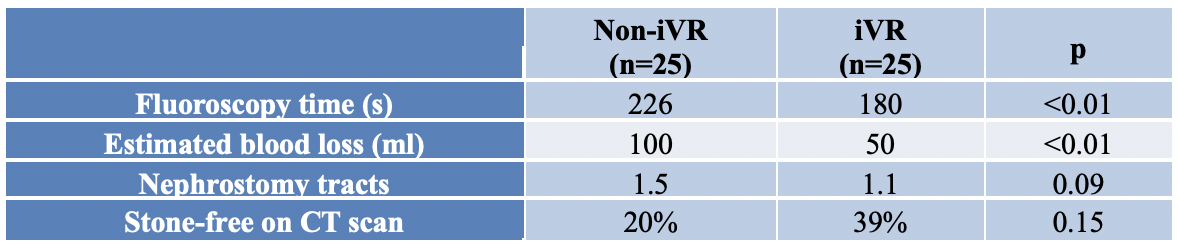
Table 1. Operative outcomes in virtual reality (iVR) and non-virtual reality (Non-iVR) groups
Authors: Egor Parkhomenko,1Mitchell O’Leary,1Shoaib Safiullah,2Sartaaj Walia,1Ryan James,3Cyrus Lin,1Roshan Patel,1Kamaljot Kaler,1Jaime Landman,1and Ralph Clayman1
Affiliation:
1Department of Urology, University of California, Irvine, Orange, CA
2Department of Urology, University of Missouri, Columbia, MO
3Department of Biomedical Informatics and Medical Education, University of Washington, Seattle, WA
Presented and Written by Francis Jefferson, Department of Urology, University of California-Irvine) at the American Urological Association's 2019 Annual Meeting (AUA 2019), May 3 – 6, 2019 in Chicago, Illinois