(UroToday.com) Dr. Hoffman-Censits concluded the session by presenting on the topic of sequencing systemic therapies and looking to the future in the management of metastatic urothelial carcinoma.
She started by talking about the current state of frontline management of metastatic urothelial carcinoma (mUC), which is platinum based chemotherapy (PBC) followed by checkpoint inhibitor maintenance therapy.
- This is supported by the JAVELIN Bladder 100 clinical trial, where patients were treated with front line PBC and were then randomized to either best supportive care (BSC) or Avelumab + BSC. The study demonstrated improved OS benefit and changed standard of care.
She delved into the cohort a bit. Most of the patients had complete or partial response to PBC (25% had stable disease). After avelumab therapy, there was an additional 10% response in patients who had stable disease or partial response to PBC.
But there was a proportion of patients that had progression on avelumab maintenance – and these patients very quickly demonstrated resistance to IO treatment and need alternative treatment approaches.
She highlighted the many abstracts and talks at this meeting discussing real-world utilization and experiences with the Avelumab maintenance therapy.

They have reinforced the survival benefit of avelumab maintenance – but uptake has not been great in the community. Patients with liver metastases seem to have the poorest response to maintenance.
But, interestingly there has also been increased uptake of carboplatin based chemotherapy – whereas they previously would have gotten checkpoint inhibitor therapy upfront.
There are some key ongoing chemotherapy and maintenance trials. She highlighted these two:

- DISCUS trial can help guide the discussion re: de-escalation of therapy
- MAIN-CAV looks at combination cabo/avelumab vs. avelumab alone
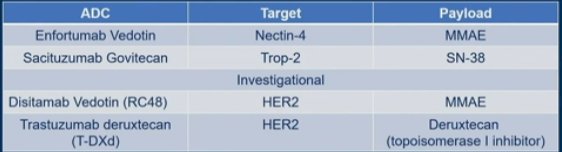
In the next line setting, we begin to look at antibody-drug conjugates (ADCs), of which there are 3:
- Enfortumab Vedotin (EV) – FDA approved
- Sacituzumab Govitecan (SG) – FDA approved
- Novel HER-2 directed ADC - investigational
Their targets and chemotherapy payloads are summarized here:
So, what is the right sequence of these therapies? At this point time, most are using these therapies dogmatically – PBC (cisplatin or carboplatin), IO maintenance if clinical benefit, then ADC. EV has been used for a long time, which has generated a lot of data to potentially help guide the though process.
The UNITE dataset is a large multi-institutional collaborative looking at the real world use of these various therapies in patients with metastatic UC. Several abstracts at the meeting looking at EV outcomes from this dataset.
Abstract 514 (Koshkin V et al) looked at whether the last therapy before EV use affect outcomes? Of 247 patients, 186 were treated with ICI prior while 61 were treated with PBC prior. It seemed that patients treated with ICI prior to EV had better ORR, mPFS and mOS.
Does the EV sequence with CPI impact skin toxicity grade? In a study by Dr. Srinivas and her dermatology colleagues (Molina GE et al. EU 2023), patients treated with ICI prior to EV had much higher levels of skin toxicity (including Grade 3-4) – likely due to some priming by ICI.
Interestingly, in a study by Dr. Hoffman-Censits group out of Johns Hopkins (Vachou et al. EU Open Science 2023), those same patients with skin toxicity had higher response rates – suggesting, it may be a marker of response.
Next, with regards to ADC Targets and Payloads, since there is some overlap, is cross-resistance a concern?
Looking at EV followed by SG, the TROPHY study provides some information. In the TROPHY-U-01 Cohort 1 (progressive disease despite PBC and checkpoint inhibition), 8.8% of patients had prior EV. 3/10 had partial response to SG (reflective on entire population), while 2/3 had best response of PD to prior EV. In the Cohort 2 (progressive disease to ICI, but platinum ineligible), 18% received prior EV. Results pending.
In the real world dataset (Hopkins, Abstract 523), 18 patients had EV followed by SG (either directly after or with intervening therapies). 4 quickly decline and 1 pending scans. However, of the remaining 13, PFS was 2.5 months, clinical benefit (CR+PR+SD) was 46.2%.
Unfortunately, regarding sequencing EV after SG, there is really no data for this yet. But with SG being used in earlier line settings, this data is likely coming.
With regards to ADC and IO combinations, below is a summary slide of some combinations. Cannot compare, as these are in different lines of therapy.
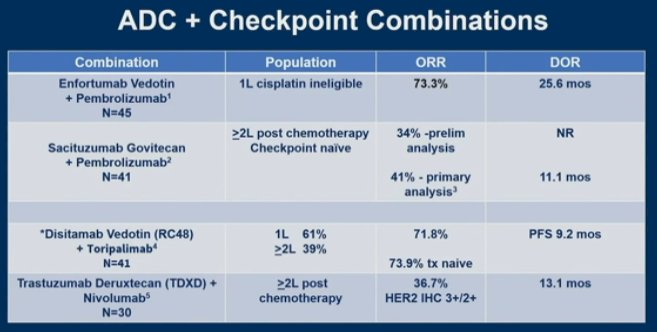
There are 2 large ADC+IO front line Phase III trials are ongoing:

EV-302 is completed and is pending report.
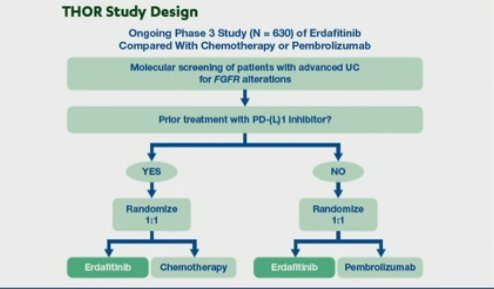
She finally touched on targeted oral therapy – specifically Erdafitinib, a targeted oral FGFR3-inhibitor. The ongoing THOR study may help to understand the role of this medication better. It compares Erdafitinib against PBC and IO therapy in patients with FGFR3 alterations.
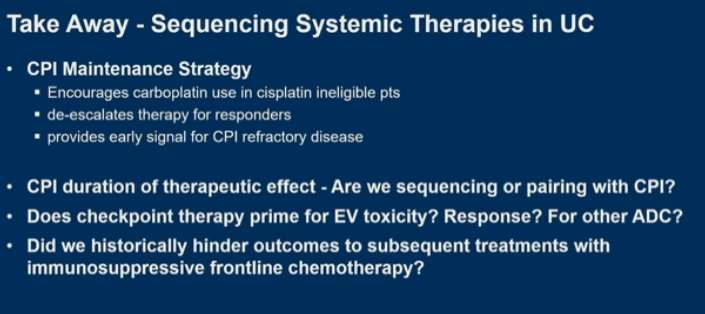
She ended with the following slide, which highlights some take home points about sequencing and some questions that still need to be answered:
Presented by: Jean H. Hoffman-Censits, MD, Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
Written by: Thenappan (Thenu) Chandrasekar, MD – Urologic Oncologist, Associate Professor of Urology, University of California, Davis @tchandra_uromd on Twitter during the 2023 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, Thurs, Feb 16 – Sat, Feb 18, 2023.