(UroToday.com) Dr. Kates, as the second talk of this session of Innovations and Multidisciplinary Care in Early- and Late-Stage Urothelial Cancer, focused on Next-Generation Therapies in Nonmuscle-Invasive Bladder Cancer (NMIBC).
He started off by highlighting the rapid changes in the field and management of NMIBC, including recent trials that have enabled new treatment options in this disease space. In this slide (provided by Dr. Noah Hahn), they highlight some key trials in this disease space:
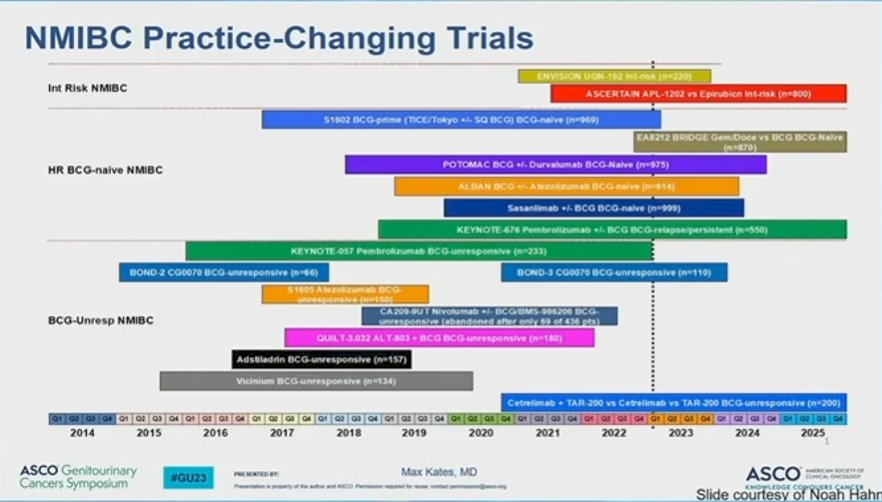
He organized the talk by NMIBC risk groups – for the following reason: each risk group has a different SOC that serves as the comparator arm.
- Low risk disease: Surveillance
- Intermediate risk disease: TURBT (in the neoadjuvant setting) vs. intravesical chemo (in the adjuvant setting)
- High risk disease: BCG
- BCG Unresponsive High Risk Disease: Cystectomy
He then showed an equation he has shown before to underscore what clinicians are looking for in new therapies – and what we may be comfortable with. Specifically, the equation is:
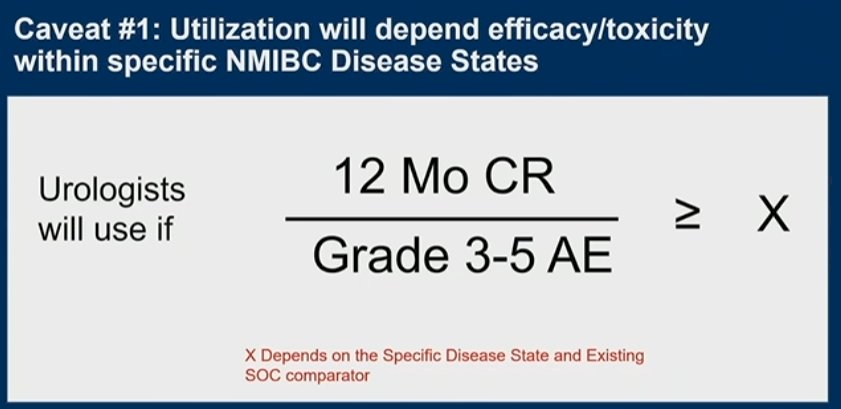
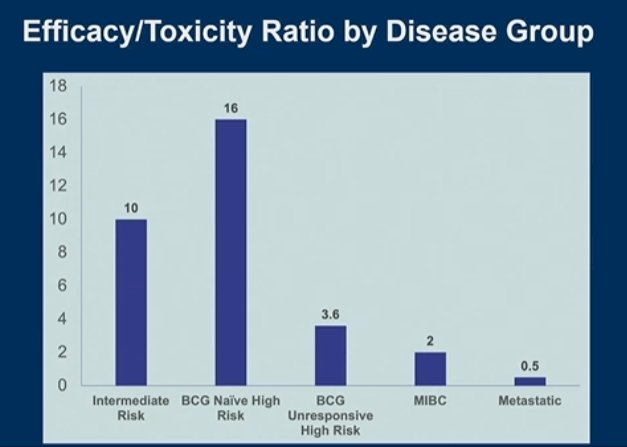
The cutoff is a moving target and depends on both the disease state and the existing comparator. This can be seen below, where he uses the current 12 Mo CR rates of known SOC.
He started with Intermediate Risk Disease (recurrent LG Ta, LG Ta > 3 cm, multifocal LG Ta). TURBT remains the standard of care therapy comparator – but while we often consider it benign, it isn’t benign for patients. It carries risks, especially if repeated multiple times. So, any therapies that can reduce or replace TURBT, that would be a benefit to patients.
Over the past 5-7 years, there has been a growth in innovations to improve intravesical delivery (mechanical devices, hydrogels, nanoparticles, etc). He highlighted an example of one method, specifically UGN-102 which is a mitomycin hydrogel.1 This demonstrated a 65% CR at 3 months, and of these patients, 95%, 73% and 61% remained disease-free at 6, 9 and 12 months after treatment initiation, respectively. In doing so, this significantly reduced burden of repeated TURBTs.
But, there is also systemic therapies being explored. An ongoing study of 30 days of oral Pemigatinib (FGFR3 inhibitor) by Noah Hahn and colleagues is exploring its use in early stage NMIBC, especially since FGFR3 mutations are enriched in NMIBC disease.
Looking next at high risk disease, the comparator arm is BCG. He notes that BCG works better than historically reported, as seen in contemporary studies.2 In the NIMBUS trial, 1-year RFS for standard dose BCG was 89% - and still ~65% for reduced frequency BCG.
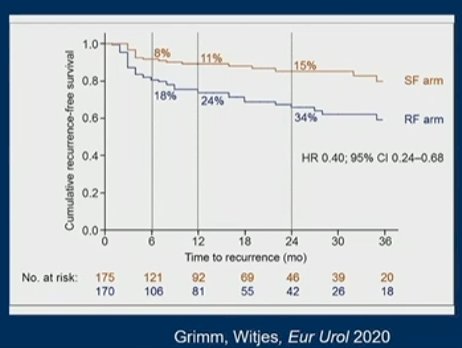
So, then how do we compete with those numbers? We don’t! We need to find alternatives as BCG shortage has necessitated it. This includes trials to establish alternative sources to the TICE BCG strain we depend on (SWOG 1602 PRIME trial, evaluating TICE vs. Tokyo strain BCG) or replace BCG altogether. SWOG 1802 has already enrolled 1000 patients and results are pending.
He then addressed the EA8212 BRIDGE Trial – a randomized Phase III Trial of BCG vs. Intravesical Gem/Doce in the BCG naïve setting. The trial parameters are seen below and they are actively recruiting sites and patients:
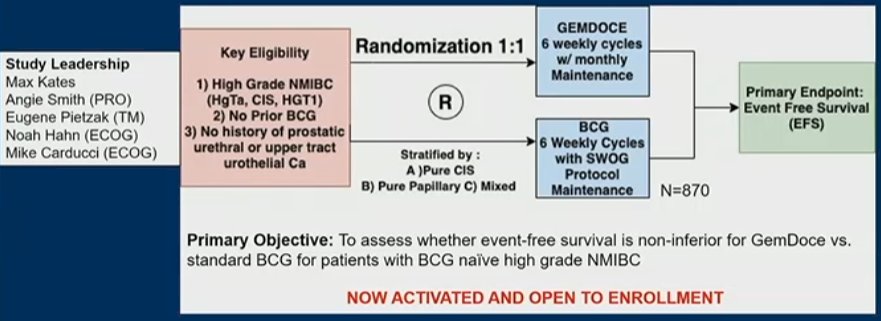
It should be noted though that the study requires full dose BCG (supplied by the institution) to activate – and that has been a limiting factor for many.
He highlighted the Phase II study lead-in to the above Phase III trial – in that Phase II study (being presented at the meeting), they found a 3-month 100% CR rate and 12-month 82% CR rate in 25 patients.
Finally he finished with the BCG Unresponsive High Risk NMIBC category. The comparator is cystectomy. There are now intravesical, systemic and combination therapies now available. But, there remains a clinical need for additional therapies that may be able to move into the front line.
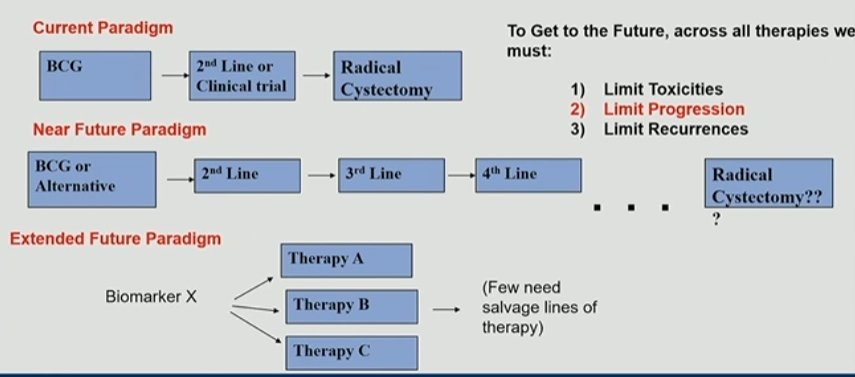
The current paradigm doesn’t include many options – BCG, one salvage therapy, then cystectomy.
However, with the new approvals, patients may be able to cycle through multiple sequential salvage therapies – but we have to balance that against toxicity, recurrences and repeat TURBTs, and risk of progression. Ideally, we get to a biomarker driven pathway that limits the need for salvage therapies.
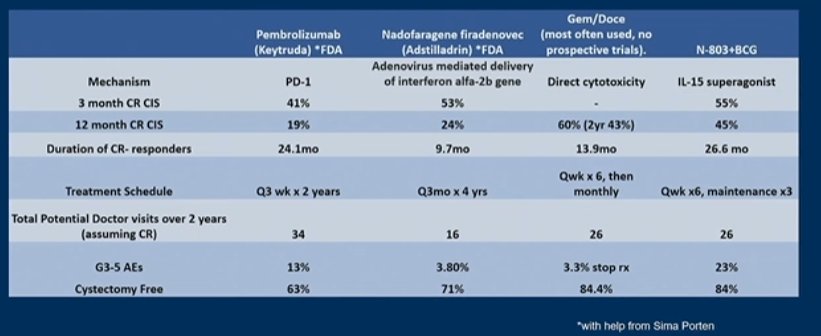
Below is the landscape (not comprehensive) of treatment options:
Presented by: Max R. Kates, MD, James Buchanan Brady Urological Institute, Johns Hopkins University School of Medicine
Written by: Thenappan (Thenu) Chandrasekar, MD – Urologic Oncologist, Associate Professor of Urology, University of California, Davis @tchandra_uromd on Twitter during the 2023 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, Thurs, Feb 16 – Sat, Feb 18, 2023.
References:
- Chevli KK, Shore ND, Trainer A, Smith AB, Saltzstein D, Ehrlich Y, Raman JD, Friedman B, D'Anna R, Morris D, Hu B, Tyson M, Sankin A, Kates M, Linehan J, Scherr D, Kester S, Verni M, Chamie K, Karsh L, Cinman A, Meads A, Lahiri S, Malinowski M, Gabai N, Raju S, Schoenberg M, Seltzer E, Huang WC. Primary Chemoablation of Low-Grade Intermediate-Risk Nonmuscle-Invasive Bladder Cancer Using UGN-102, a Mitomycin-Containing Reverse Thermal Gel (Optima II): A Phase 2b, Open-Label, Single-Arm Trial. J Urol. 2022 Jan;207(1):61-69. doi: 10.1097/JU.0000000000002186. Epub 2021 Aug 26. PMID: 34433303; PMCID: PMC8667793.
- Grimm MO, van der Heijden AG, Colombel M, Muilwijk T, Martínez-Piñeiro L, Babjuk MM, Türkeri LN, Palou J, Patel A, Bjartell AS, Caris C, Schipper RG, Witjes WPJ; EAU Research Foundation NIMBUS Study Group. Treatment of High-grade Non-muscle-invasive Bladder Carcinoma by Standard Number and Dose of BCG Instillations Versus Reduced Number and Standard Dose of BCG Instillations: Results of the European Association of Urology Research Foundation Randomised Phase III Clinical Trial "NIMBUS". Eur Urol. 2020 Nov;78(5):690-698. doi: 10.1016/j.eururo.2020.04.066. Epub 2020 May 20. PMID: 32446864.