(UroToday.com) The 2022 GU ASCO Annual meeting included a session on the optimization management of localized prostate cancer, specifically looking at artificial intelligence (AI), active surveillance, and intervention, featuring a presentation by Dr. Alberto Bossi discussing the changing horizons of radiation therapy in localized disease. Dr. Bossi started by highlighting that we need better use of established technologies, dissemination of new technologies, answers to old questions, and a patient-centered approach to radiotherapy.
Dr. Bossi first discussed FLAME, a phase III,1 multicenter, randomized controlled Focal Lesion Ablative Microboost in Prostate Cancer (FLAME) trial of 571 patients with intermediate- and high-risk prostate cancer. Patients were assigned to standard treatment of 77 Gy (fractions of 2.2 Gy) to the entire prostate. The focal boost arm received an additional simultaneous integrated focal boost up to 95 Gy (fractions up to 2.7 Gy) to the intraprostatic lesion visible on mpMRI. The primary endpoint for FLAME was 5-year biochemical disease-free survival (DFS). Over a median follow-up of 72 months, biochemical DFS was significantly higher in the focal boost arm compared with the standard arm (HR 0.45, 95% CI, 0.28 to 0.71):
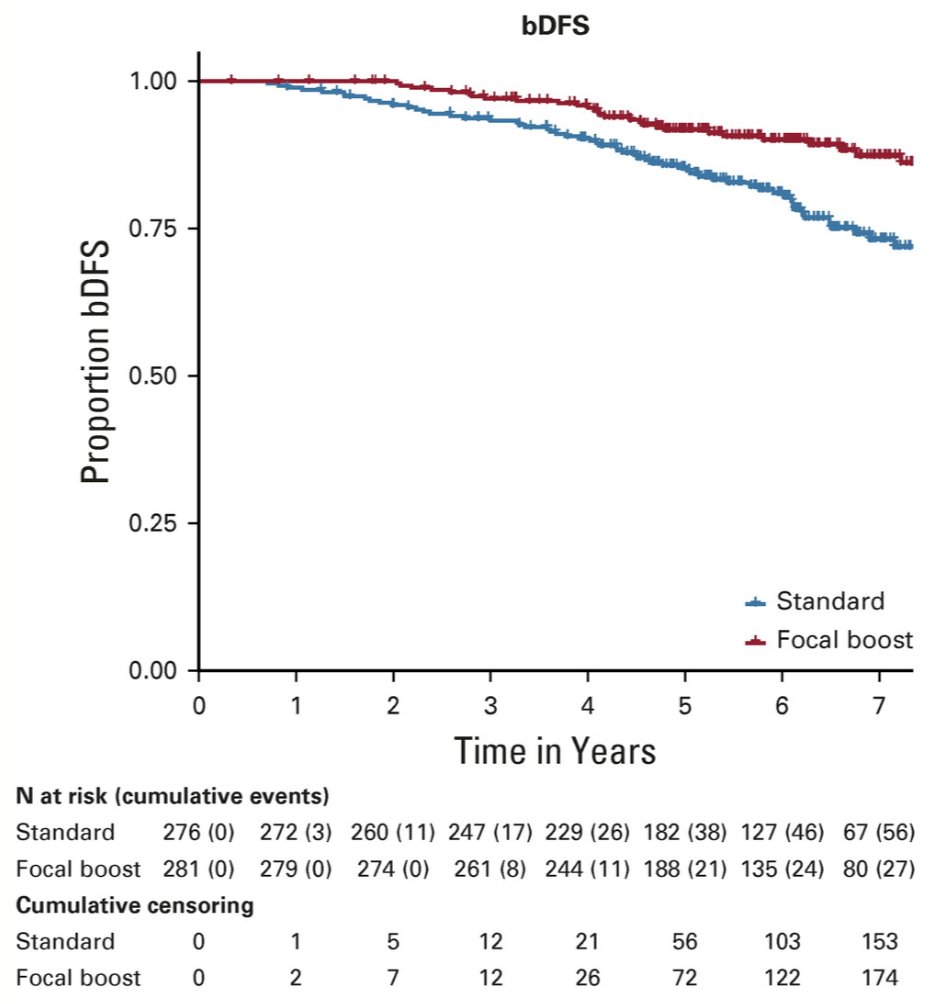
At 5-year follow-up, biochemical DFS was 92% and 85%, respectively; there were no differences in prostate cancer-specific survival (p = 0.49) and overall survival (p = 0.50). The cumulative incidence of late genitourinary and GI toxicity grade ≥ 2 was 23% and 12% in the standard arm versus 28% and 13% in the focal boost arm, respectively.
Dr. Bossi notes that it is important to understand the optimal minimum duration of ADT when treating high risk prostate cancer with high-dose radiotherapy. Kishan et al.2 recently published a patient-level data analysis of 3 cohorts assessing ADT and external beam radiotherapy with or without brachytherapy boost for optimal treatment of high-risk prostate cancer. Among 3,410 men with high-risk prostate cancer, there was a significant interaction between the treatment type (external beam radiotherapy vs external beam radiotherapy + brachytherapy) and ADT duration (<6, 6 to <18, and ≥18 months). The minimum duration threshold for ADT was 26.3 months (95% CI, 25.4-36.0 months) for external beam radiotherapy and 12 months (95% CI, 4.9-36.0 months) for external beam radiotherapy + brachytherapy for optimal effect on distant metastasis free survival:

Dr. Bossi notes that recent interest has been related to intense radiotherapy fractionation. The Scandinavian HYPO-RT-PC randomized controlled phase III trial3 randomized men with intermediate and high-risk prostate cancer to either conventional fractionating (n = 602; 78.0 Gy in 39 fractions, 5 days per week for 8 weeks) or ultrahypofractionated (n=598; 42.7 Gy in seven fractions, 3 days per week for 2.5 weeks). The primary endpoint was time to biochemical or clinical failure. The estimated failure-free survival at 5 years was 84% (95% CI 80-87) in both treatment groups, with an adjusted HR of 1.002 (95% CI 0.758-1.325; log-rank p=0.99). There was weak evidence of an increased frequency of acute physician-reported RTOG grade 2 or worse urinary toxicity in the ultra-hypofractionation group at end of radiotherapy (158 [28%] of 569 patients vs 132 [23%] of 578 patients; p=0.057). Based on these results, there has been support for the use of ultra-hypofractionated radiotherapy for prostate cancer.
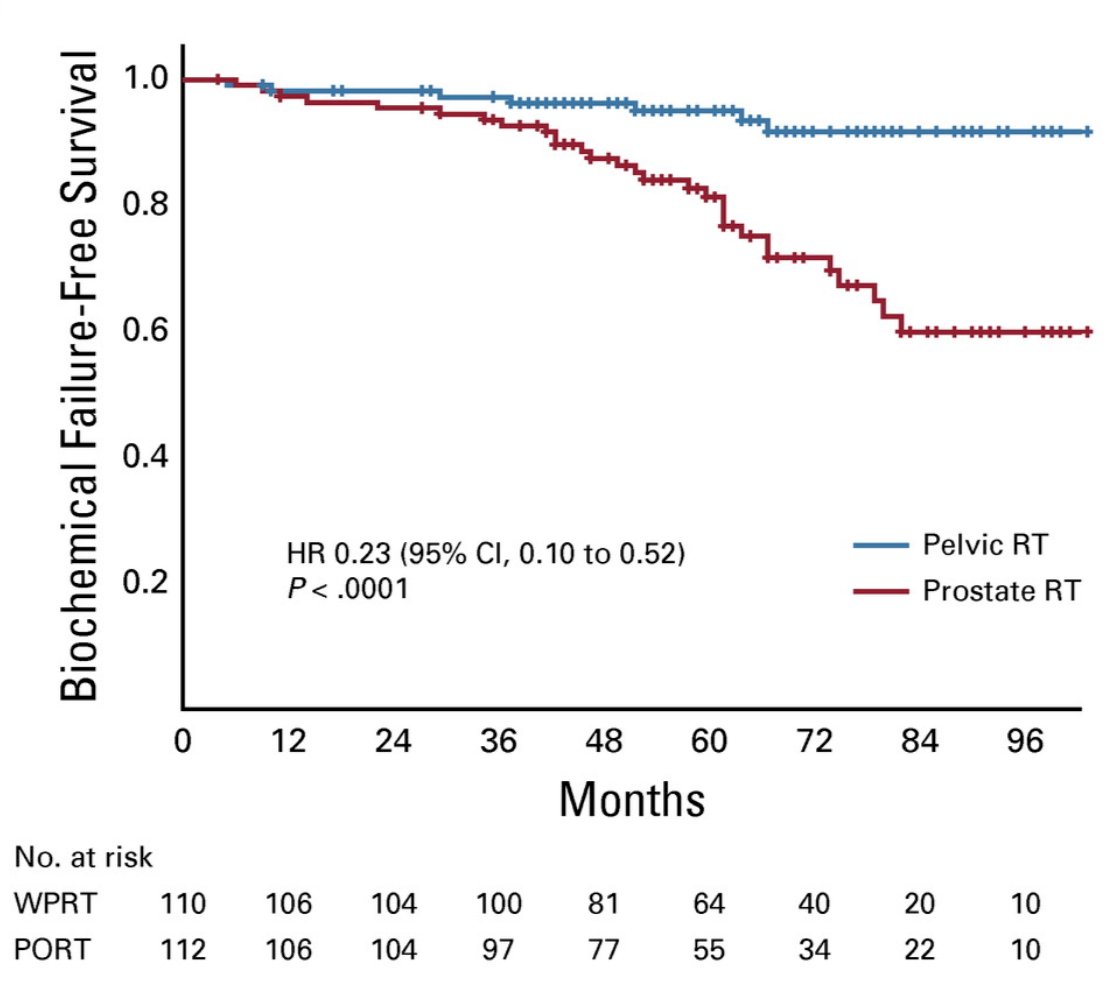
Dr. Bossi then discussed the POP-RT trial,4 which was a randomized trial comparing prophylactic whole-pelvic nodal radiotherapy to prostate-only radiotherapy in high-risk prostate cancer. In this phase III trial, men were enrolled who were undergoing radical radiotherapy for node-negative prostate cancer, with estimated nodal risk ≥ 20%. Randomization was 1:1 to prostate-only radiotherapy (68 Gy in 25 fractions to prostate) or whole-pelvic radiotherapy (68 Gy in 25 fractions to prostate, and 50 Gy in 25 fractions to pelvic nodes, including common iliac). All patients received image-guided, intensity-modulated radiotherapy and minimum 2 years of ADT. The primary endpoint was 5-year biochemical failure-free survival. A total of 224 patients were randomly assigned and at a median follow-up of 68 months, 5-year biochemical failure-free survival was 95.0% (95% CI, 88.4 to 97.9) with whole-pelvic radiotherapy versus 81.2% (95% CI, 71.6 to 87.8) with prostate-only radiotherapy (aHR 0.23, 95% CI 0.10 to 0.52):
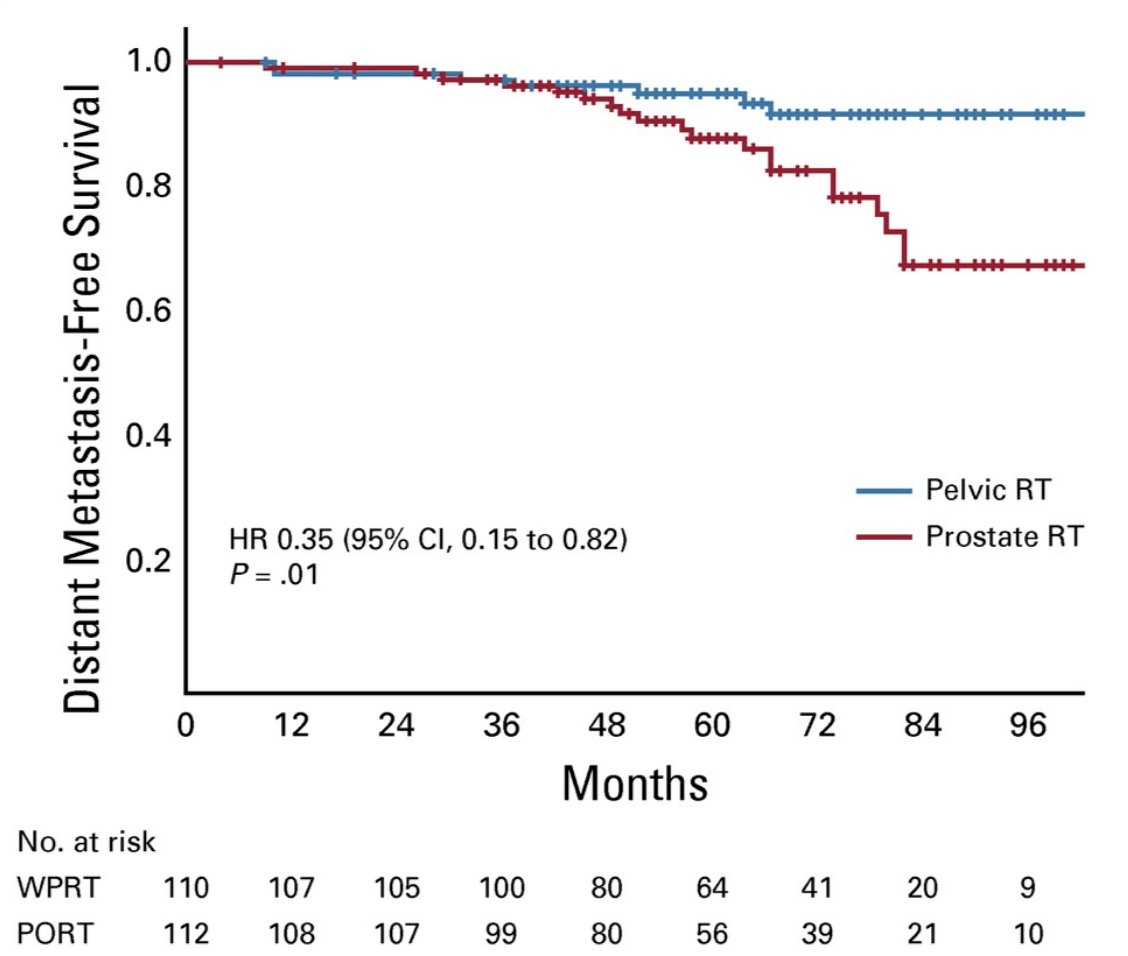
Distant metastasis-free survival was also higher with whole-pelvic radiotherapy (95.9% vs 89.2%; HR 0.35; 95% CI, 0.15 to 0.82):
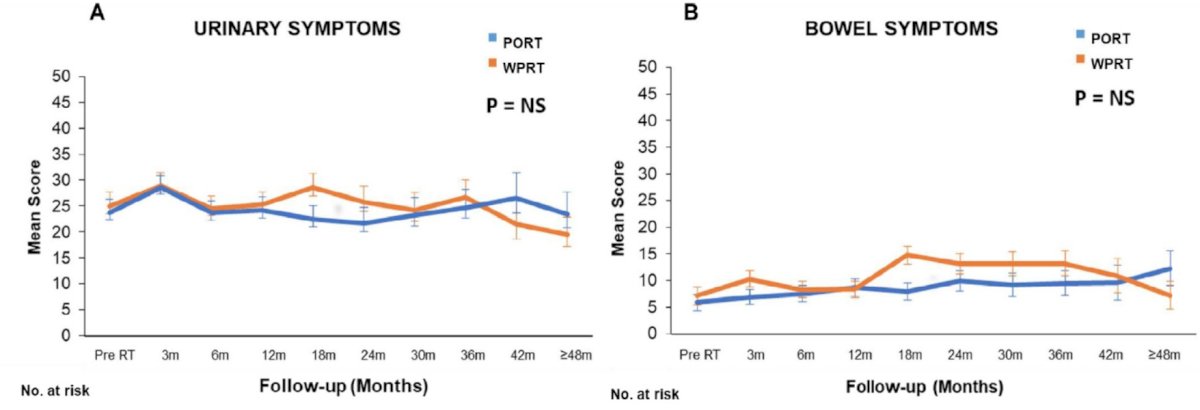
Additionally, a modest increase was observed in the incidence of grade ≥ 2 late genitourinary toxicity with pelvic radiotherapy, with a low incidence of GI toxicity in both the arms:
Dr. Bossi notes that there is a “sliding window” of whole-pelvic radiotherapy, weighing the balance of probability of a “pure” intraprostatic disease versus the probability of metastatic disease. To improve appropriate treatment for these patients, he recommends utilization of the Roach formula and pre-treatment PSMA imaging:

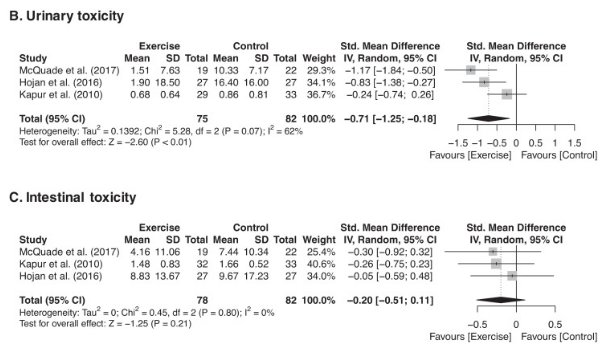
Finally, a patient centered approach must take into account toxicity of treatment for the patient. Schumacher et al.5 assessed the effects of exercise during radiation therapy on physical function and treatment-related side effects in men with prostate cancer, noting that among 391 men included in this review, exercise resulted in consistent significant benefits for physical function in terms of cardiovascular fitness and muscle function. Additionally, there was a significant positive effect of exercise on urinary toxicity, but not on intestinal or hormonal toxicity, depression, or sleep symptoms:
Dr. Bossi concluded his presentation of the changing horizons of radiation therapy in localized disease noting that we should utilize focal mpMRI guided radiotherapy boosts, external beam radiotherapy should be utilized with brachytherapy boosts, extreme hypofractionation has arrived for appropriately selected patients, and consideration should be given for pelvic lymph node irradiation in men at high risk for nodal involvement. Ultimately, we are striving for precision and personalization of radiotherapy.
Presented by: Alberto Bossi, MD, Gustave Roussy, Institute, Paris, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, Thursday Feb 17 – Saturday Feb 19, 2022
References:
- Kerkmeijer LGW, Groen VH, Pos FJ, et al. Focal boost to the intraprostatic tumor in external beam radiotherapy for patients with localized prostate cancer: Results from the FLAME randomized phase III trial. J Clin Oncol. 2021 Mar 1;39(7):787-796.
- Kishan AU, Steigler A, Denham, et al. Interplay between duration of androgen deprivation therapy and external beam radiotherapy with or without brachytherapy boost for optimal treatment of high-risk prostate cancer: A Patient-level data analysis of 3 cohorts. JAMA Oncol. 20 Jan 2022 [Epub ahead of print].
- Widmark A, Gunnlaugsson A, Beckman L, et al. Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial. Lancet. 2019;394(10196):385-395.
- Murthy, V, Maitre P, Kannan S, et al. Prostate-only versus whole-pelvic radiation therapy in high-risk and very high-risk prostate cancer (POP-RT): Outcomes from phase III randomized controlled trial. J Clin Oncol. 2021;39:1234-1242.
- Schumacher O, Luo H, Taaffe DR, et al. Effects of exercise during radiation therapy on physical function and treatment-related side effects in men with prostate cancer: A systematic review and meta-analysis. Int J Radiat Oncol Biol Phys. 2021 Nov 1;111(3):716-731.