To begin, the only Level 1 evidence supporting the oncologic efficacy PN compared to RN is the EORTC study by van Poppel et al. (EU 2007). However, it was underpowered and had significant cross-over. Comparative efficacy literature outside of this trial is limited to observational studies with inherent selection bias and unmeasured confounding. At this time, based on this literature, the guidelines support the use of PN as the standard of care for small renal mass (cT1a lesions) but offer either PN or RN for pT1b and more complex lesions.
Dr. Psutka accepts that there are cases of complex renal masses >= pT1b lesions that are obligate for PN –solitary kidneys, bilateral renal masses, etc. However, what she is here to argue for today is the use of ePN in situations where it isn’t obligate –like the picture below:
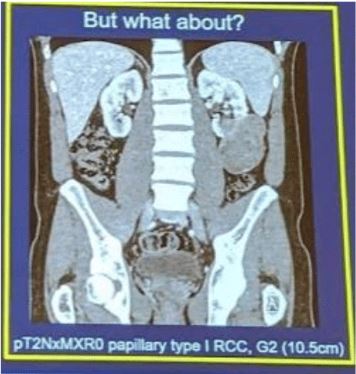
These are larger tumors and potentially endophytic but in the setting of a solitary tumor, normal contralateral kidney, and normal renal function.
Yet, she is not being cavalier –she understands that this needs to be done safely.
The conditions for pushing surgical boundaries are as follows:
- Feasibility and safety, including oncologic outcomes
- A demonstrated benefit to the patient
1. Perioperative outcomes
In the study by Mir et al., they found no differences in operative time, ~100 cc higher blood loss (arguably not clinically significant) –but did note a slightly higher risk of postoperative complications (HR 1.74). Yet, this did not translate to a higher 30-day or 90-day mortality –as there was no difference between the two groups.
An et al. (Urology 2017) specifically looked at this question in the elderly population and found no difference in postoperative complication rates (~38%) or urologic complications (~40%), p > 0.05.
2. Oncologic efficacy
Again, in the Mir et al. study, on meta-analysis, tumor recurrence (HR 0.58) and disease-free survival (HR 0.60) were superior in the PN cohort –though, considering most of the studies were retrospective, these were likely compromised to some degree by selection bias. However, she notes that, in well-selected patients, tumor recurrence rates and cancer-specific survival are high.
In a study by Hansen et al. (Urology 2012), they found that, on multivariable analysis, there was no significant difference in oncologic outcomes for tumors > 7 cm, tumors with FG 3-4, and for stage pT3a tumors (p = 0.2, 0.2, 1.0, respectively).
3. Preservation of renal function
There is no argument that PN preserves nephrons better than an RN does. In a longer-term follow-up of the EORTC study (Leppert et al., J Am Soc Neph 2018), in patients with baseline eGFR >30 and > 45, the incidence of CKD stage 4 was significantly higher in patients undergoing RN than patients undergoing PN –(9.6% vs. 4.2% in patients with eGFR > 30, 20.1% vs. 3.7% in patients with eGFR > 45 at baseline).
4. Associated decreased risk of CV events
A few prior studies have demonstrated an associated risk of decreased CV morbidity with patients undergoing PN.
5. Overall survival
In a study by Tan et al. (JAMA 2012), in older patients with kidney cancer, PN was associated with lower overall cause mortality (HR 0.54).
Specifically, in a propensity-matched analysis of pT1b tumor patients undergoing ePN vs. RN, Venkatramani et al. (Urol Onc 2018), found that overall survival favored patients undergoing ePN (HR 0.78). Similar results were seen in work by Kim et al. (J Urol 2012) and Mir et. al.
6. Quality of Life Poulakis et al. (Urology 2003) demonstrated that PN (vs. RN) is associated with better physical function and global QOL, and higher QOL at 3 and 12 months with improvement over time.
Parker et al. (J Urol 2012) demonstrated that QOL improves with higher postoperative eGFR –and as prior studies have shown, that is better achieved with PN.
Based on all of this, Dr. Psutka argues that ePN should be a viable option –but in selected patients! She isn’t saying every patient with T1b/T2 tumors should get ePN –but it should be considered, and if deemed to be safe, completed.
In a study by Kopp et al. (Urology 2015), they found that nephrometry score was associated with oncologic outcomes, independent of tumor stage. De novo CKD was significantly lower with ePN vs. RN in patients with a nephrometry score between 6-8 –but no difference in patients in scores 9-10.
Her conclusion slide was nice and hit all the main points:
Dr. Van Poppel gave the rebuttal –supporting RN.
Presented by: Sarah P. Psutka, MD, MS, University of Washington Medical Center, Seattle, Washington
Written by: Gina B Carithers Founder and Publisher at UroToday.
Written by: Thenappan Chandrasekar, MD(Clinical Instructor, Thomas Jefferson University, Philadelphia, Pennsylvania, twitter: @tchandra_uromd, @JEFFUrology at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA