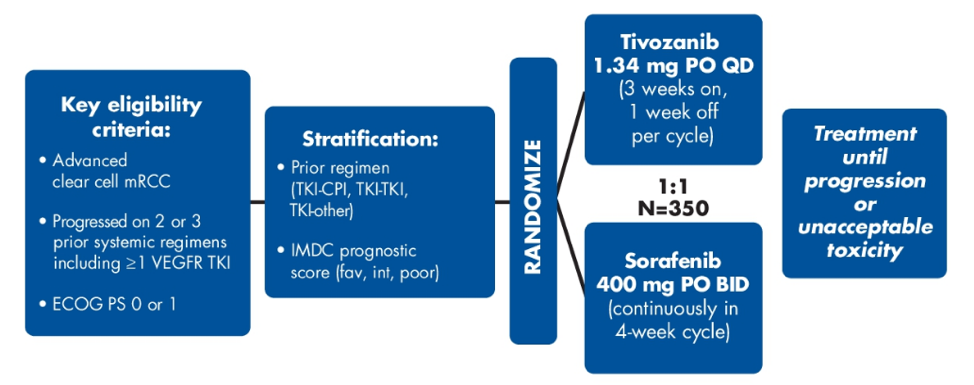
The TIVO-3 study enrolled subjects with metastatic RCC who failed 2 or 3 prior systemic regimens, one of which included a VEGFR TKI, stratified by IMDC risk category and type of prior therapy (two TKIs; TKI plus checkpoint inhibitor therapy; TKI + other) and then randomized patients 1:1 to tivozanib versus sorafenib. The TIVO-3 trial design is as follows:
The primary endpoint was PFS and secondary endpoints included OS, overall response rate, duration of response, and safety. The data cutoff for this analysis was January 15, 2021. There were 41 responders (23%) to tivozanib and 20 responders (11%) to sorafenib with the overall response rate highlighted in the following table:

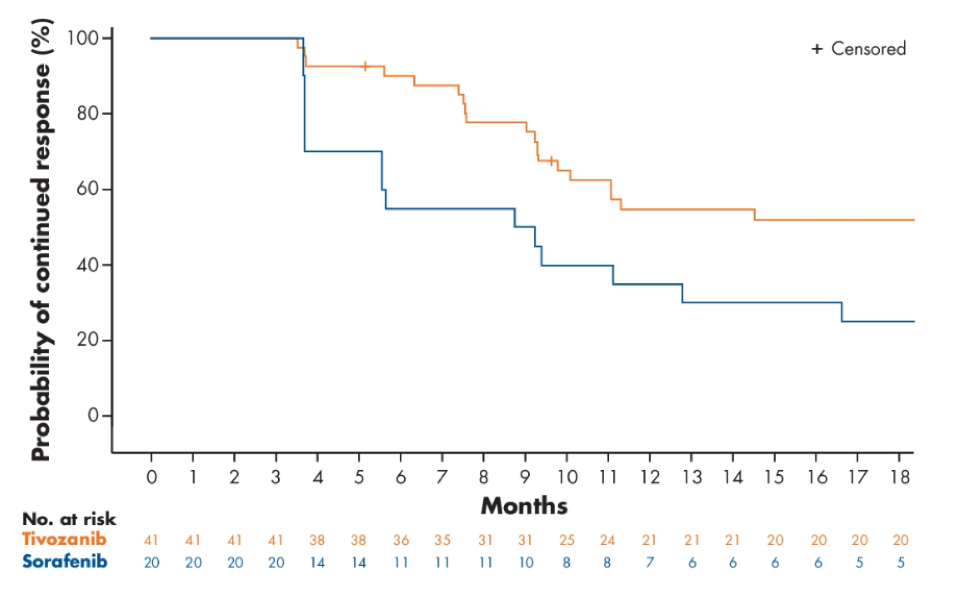
The median duration of response was 20.3 months (95% CI 9.8 to 29.9) and 9.0 months (95% CI 3.7 to 16.6) for tivozanib and sorafenib, respectively. There were 3 patients in the sorafenib arm and 13 patients in the tivozanib arm that continued to have an ongoing response at the time of data cutoff:
With prolonged follow-up there were 270 deaths, with the hazard ratio for overall survival favoring tivozanib at 0.91 (95% CI: 0.716, 1.165) but without reaching statistical significance:

Dr. Verzoni concluded her presentation of the updated analysis of the TIVO-3 trial with the following conclusions:
- Tivozanib demonstrated clinically meaningful and statistically significant improvement in overall response rate and duration of response with similar overall survival to sorafenib in patients with highly relapsed or refractory metastatic RCC
- Median duration of response was 20.3 months with tivozanib, twice that observed with sorafenib
- Statistically significant improvement in PFS and overall response rate had previously been shown and continues to improve with longer follow-up
- Overall survival relative to sorafenib continues to improve with longer follow-up
- Collectively, these data confirm and extend previous findings for tivozanib as an evidence-based treatment option for patients with relapsed and refractory RCC, including patients whose disease has progressed after previous checkpoint inhibitor therapy
Clinical trial information: NCT02627963
Presented by: Elena Verzoni, MD, Fondazione IRCCS Istituto Nazionale Tumori, Milan, Italy
Co-Author: Bernard Escudier, Thomas E. Hutson, David F. McDermott, Sumanta K. Pal, Camillo Porta, Brian I. Rini, Michael N. Needle, Michael B. Atkins; Gustave Roussy, Villejuif, France; Texas A&M College of Medicine, Bryan, TX; Beth Israel Deaconess Medical Center, Dana-Farber/Harvard Cancer Center, Boston, MA; Department of Medical Oncology & Therapeutics, City of Hope Comprehensive Cancer Center, Duarte, CA; University of Bari 'A. Moro' and Policlinico Consorziale di Bari, Bari, Italy; Vanderbilt-Ingram Cancer Center, Nashville, TN; Aveo Oncology, Boston, MA; Georgetown Lombardi Comprehensive Cancer Center, Washington, DC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021