Retrospective data has suggested an improved outcome if short ADT is added to radiotherapy in high-relapse risk patients. The RTOG 9601 study3 demonstrated an improved overall survival (OS) at 12 years after two years of ADT plus radiotherapy in patients with persistent PSA following radical prostatectomy.
In the presented trial by Dr. Magné, the efficacy of radiotherapy was compared to that of radiotherapy + short duration ADT (6 months). The study design and inclusion criteria are shown in Figure 1. This was a randomized, open-label, multicenter phase 3 study. The patients were stratified according to:
- Investigational Site
- Intensity-modulated radiotherapy (IMRT) vs. Three Dimensional (3D) Conformal
- Radiation therapy (3D RT)
- High risk vs. low risk
- Gleason score<8
- Positive surgical margins
- PSA doubling time at relapse of more than six months
- No seminal vesicle invasion
- Metastasis-free survival (MFS)
- OS
- Acute and late toxicities
- Quality of life
 After an update in 2008, the study planned to accrue 738 patients with 369 events, with a power of 80% for 10% gain in OS. Eventually, 743 patients were randomized between 2006 and 2010 in an impressive 43 French centers. The updated median follow-up is 112 months (IQR 102-123), and the delay between radical prostatectomy and relapse was shown to be 40 months (SD 27). The baseline characteristics were similar in both trial arms.
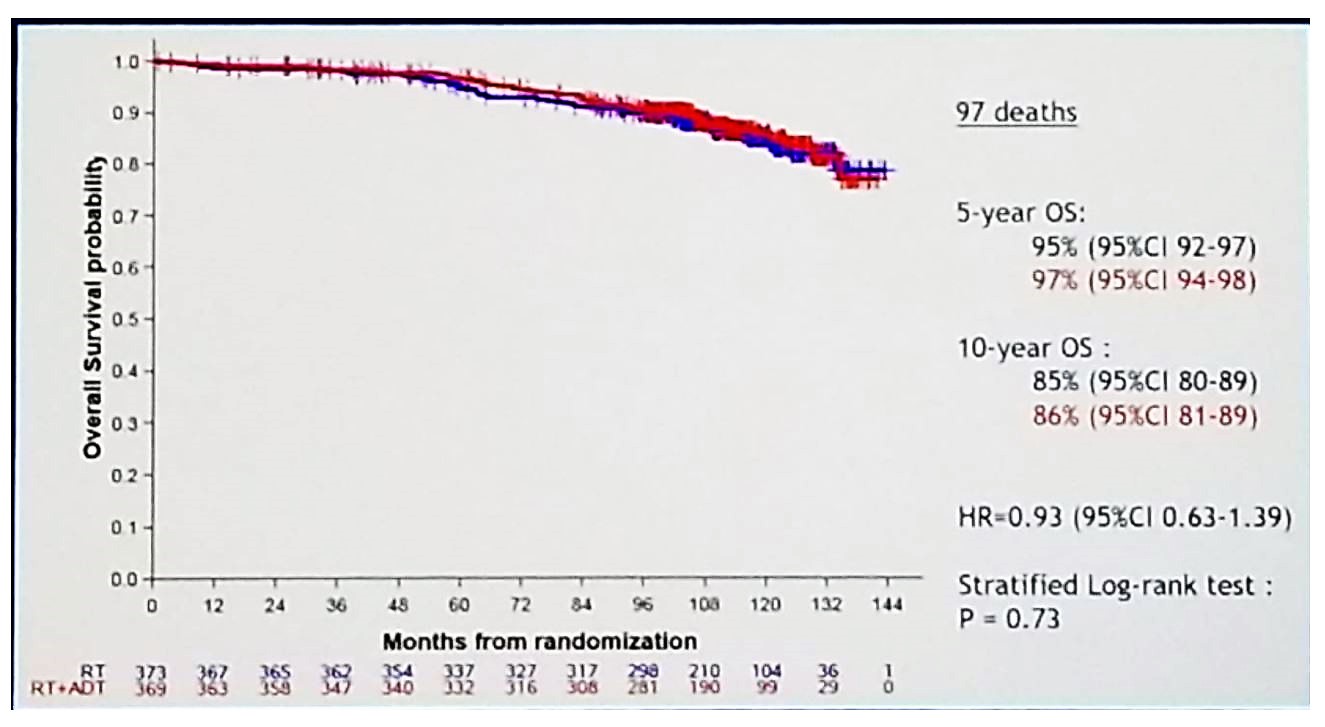
After an update in 2008, the study planned to accrue 738 patients with 369 events, with a power of 80% for 10% gain in OS. Eventually, 743 patients were randomized between 2006 and 2010 in an impressive 43 French centers. The updated median follow-up is 112 months (IQR 102-123), and the delay between radical prostatectomy and relapse was shown to be 40 months (SD 27). The baseline characteristics were similar in both trial arms.The updated PFS results in 2019 are shown in figure 2, with a clear benefit in the radiotherapy with ADT group (80% vs. 63% and 64% vs. 49% for 5- and 10-year PFS, respectively). The hazard ratio is 0.54 (95% CI 0.43-0.68, p<0.0001). The MFS also showed a benefit for the radiotherapy + ADT group, with a hazard ratio of 0.73 (95% CI 0.54-0.98), p=0.034) (Figure 3). In contrast, no difference was shown in the updated OS results (figure 4).
Figure 2 – Progression-free survival – updated 2019 results:

Figure 3- Metastasis-free survival – updated 2019 results:
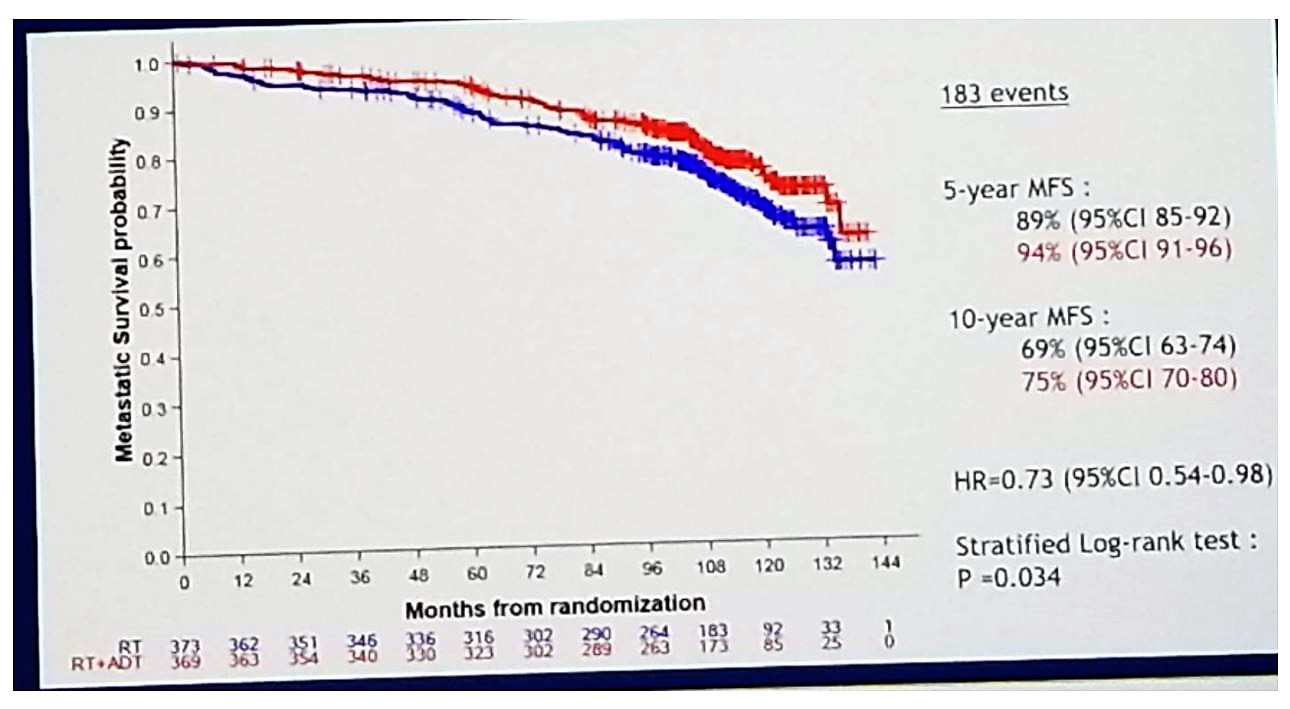
Figure 4- Overall survival – updated 2019 results:
In conclusion, short ADT combined with radiotherapy increase the 10-year MFS compared to radiotherapy alone in patients with rising PSA after radical prostatectomy. This significant improvement enables to postpone more aggressive treatment such as long-term ADT with its associated deleterious effect on patient quality of life.
Presented by: Nicolas Magné, MD, Radiotherapy Department, Centre Léon Bérard, Lyon, France
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, @GoldbergHanan at the 2019 ASCO Annual Meeting #ASCO19, May 31- June 4, 2019, Chicago, IL USA
References:
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural History of Progression After PSA Elevation Following Radical Prostatectomy. JAMA. 1999;281(17):1591–1597. doi:10.1001/jama.281.17.1591
- Stephenson AJ, Scardino PT, Kattan MW, et al. Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy. J Clin Oncol. 2007;25(15):2035–2041. doi:10.1200/JCO.2006.08.9607
- Jang et al. Int J Radiat Oncol Biol Phys 2012