This study was an open-label, randomized trial (NCT02210117), where adults with MRCC who were not previously treated with immune checkpoint therapy and anti-VEGF therapy, were enrolled and randomized in a ratio of 2:3:2 to receive either:
1. nivolumab
2. nivolumab and bevacizumab or
3. nivolumab and Ipilimumab
All patients were followed by surgery (cytoreductive nephrectomy or metastatectomy), or biopsy, and eventually received nivolumab maintenance therapy up to 2 years. All patients were assessed for response at ≥12 weeks.
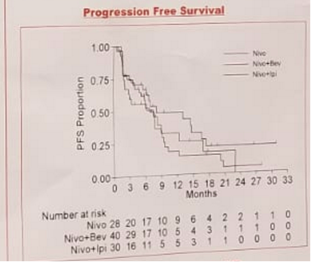
A total of 104 patients had been accrued so far, and 97 patients were evaluable for responses. Overall, 54% of the patients had complete response (CR) + partial response (PR) in the nivolumab only arm, 48% had CR+PR in the nivolumab and bevacizumab arm, and 41% had CR+PR in the nivolumab and ipilumumab arm. Out of the patients undergoing surgery, best overall response was seen in 79% of the patients in the nivolumab arm, 93% in the nivoumab and bevacizumab arm, and 69% in the nivolumab and ipilumumab arm (Figure 1 demonstrates progression free survival in all arms).
When inspecting the grade 3 or 4 toxicities, it was shown to be present in 45% of the patients in the nivolumab only arm, 56% of the nivolumab and bevacizumab arm, and 53% of the nivolumab and ipilimumab arm.
Correlative laboratory studies suggest that there are more CD8 T cell infiltration in responders as compared to non-responders.
The authors concluded that pre-surgical therapies with nivolumab +/- bevacizumab or ipilimumab were safe and showed promising clinical activities in patients with MRCC. Additionally, patients able to stay on therapy and receive surgery had best overall response, ranging from 69%-93%. The authors propose that the combination therapy of nivolumab with or without bevacizumab or ipilumumab plus cytoreductive surgery, need to be further analyzed in phase 3 trials of MRCC patients. Lastly, immune and molecular correlative studies may allow to identify novel biomarkers that can be used for correlation with clinical outcomes in patients with MRCC.
Presented by: Jianjun Gao, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter:@GoldbergHanan at the 2018 ASCO Annual Meeting - June 1-5, 2018 – Chicago, IL USA