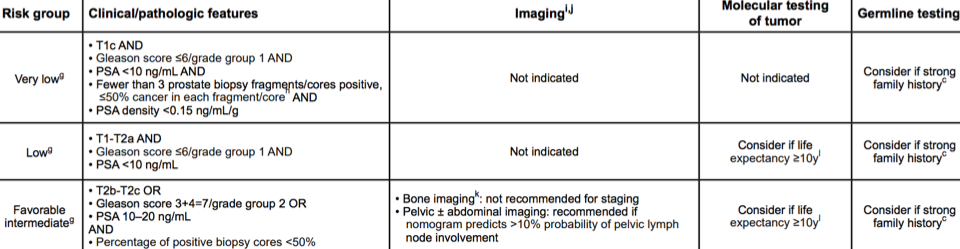
Fortunately, AS is more widely adopted in the US today, with rates as low as 10% for appropriate patients in the 1990’s, up to nearly 50% in the 2010-2013. Certainly, for NCCN very low risk men, active surveillance is standard practice, where genomics is unlikely to play a role. In the Hopkins AS cohort [1] with very low risk prostate cancer (n=926), only 2 patients (0.2%) died of prostate cancer, while 333 patients (36.0%) underwent curative treatment during follow-up.
Schaeffer feels that in the low and favorable intermediate risk groups is where genomics likely plays a role in selecting appropriate men for AS. Particularly for intermediate risk patients, appropriate identification of men for surveillance is crucial, which we have learned from several large series. In the Toronto AS series, 213 intermediate risk (60% Gleason 7) and 732 low risk cases were identified, with a median follow-up of 6.7 years for intermediate and 6.5 years for low-risk patients [2]. The 15-year metastasis-free, overall, cause-specific and treatment-free survival rates were inferior in the intermediate risk group (82% for intermediate risk vs 95% for low risk; MFS HR 3.14 95%CI 1.51-6.53). Further breakdown of the estimated 15-year MFS for cases of (i) Gleason 6 or less with PSA <10 ng/ml was 94%, (ii) Gleason 6 or less with PFS 10-20 ng/ml was 94%, (iii) Gleason 3+4 with PSA ≤20 ng/ml was 84%, and (iv) Gleason 4+3 with PSA ≤20 ng/ml or less was 63%.
Schaeffer postulates: Can precision AS improve outcomes? In his opinion, the tissue biomarkers are probably 5 years ahead of urine and blood biomarkers, and as such he primarily uses tissue biomarkers in his practice. One of the early barriers to estimating occult biological potential of prostate cancers was understanding the heterogeneity of a tumor, specifically determining if a biopsy of a tumor predicts the behavior of the “whole tumor.” We know from previous genetic studies that the lethal phenotype of prostate cancer consists of multiple genetic alterations. Previous work using the Decipher risk calculator note that genomic classifiers for aggressive disease are elevated in a small but not insignificant proportion of pure Gleason Group (GG)1 tumors, with 13% having intermediate and 7% having high-risk genomic classifier scores. Not surprisingly, Decipher metastasis score for aggressive disease are highly variable for GG2 tumors, in that 14% will have high genomic scores.
Advanced imaging, such as mpMRI, has the opportunity to further risk stratify patients appropriately for AS, particularly in the setting of a negative MRI. Dr. Schaeffer argues that targeted biopsies of men with very low risk prostate cancer has limited yield, with targeted biopsies in this setting only detecting higher grade cancer 3.9% of the time.
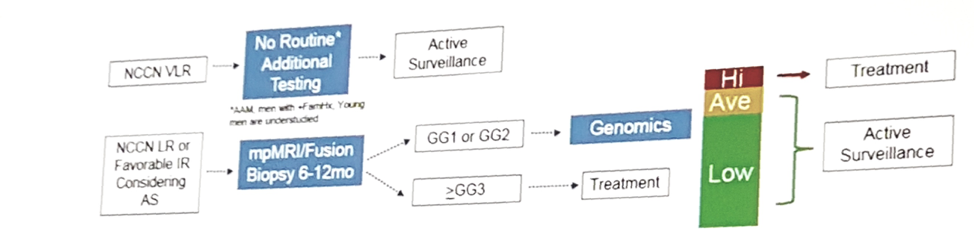
Schaeffer concluded with an elegant flow diagram of his current strategies for AS qualification:
References:
- Tosoian JJ, Mamawala M, Epstein JI, et al. Intermediate and longer-term outcomes from a prospective active-surveillance program for favorable-risk prostate cancer. J Clin Oncol 2015;33(30):3379-3385.
- Musunuru HB, Yamamoto T, Klotz L, et al. Active surveillance for intermediate-risk prostate cancer: Survival outcomes in the Sunnybrook experience. J Urol 2016;196(6):1651-1658.
Presented by: Edward Schaeffer, MD, Department of Urology, Northwestern University Feinberg School of Medicine, Chicago, IL
Written by: Zachary Klaassen, MD, Urologic Oncology Fellow, University of Toronto, Princess Margaret Cancer Centre, Twitter: @zklaassen_md at the 2018 ASCO Annual Meeting - June 1-5, 2018 – Chicago, IL USA