(UroToday.com) The 2022 Advanced Prostate Cancer Consensus Conference (APCCC) Hybrid Meeting included a session on the management of metastatic hormone sensitive prostate cancer (mHSPC), and a presentation by Dr. Gert Attard discussing whether we need more granularity in mHSPC and whether biology can help with treatment decisions. To start his presentation, Dr. Attard asked the question: Outside of a clinical trial, would the information on tumor genomic profiling (primary tumor or metastatic lesion) influence your first-line treatment decision of mHSPC? There are several mHSPC trials implementing molecular biomarkers that are either recruiting already or being planned:
- BRCA2/DRD: AMPLITUDE (NCT037486641), TALOPRO-3 (NCT04821622), and STAMPEDE
- PTEN loss: CAPItello-281 (NCT04493853)
- PSMA positive: PSMAddition (NCT04720157)
- Cell cycle: CYCLONE 3 testing abiraterone + prednisone +/- LY2835219
Dr. Attard notes that in the STAMPEDE arm of high-risk localized prostate cancer treated with either abiraterone or enzalutamide, there was a consistent effect with ARPI regardless of metastatic burden.1 In this study, local radiotherapy (as per local guidelines, 74 Gy in 37 fractions to the prostate and seminal vesicles or the equivalent using hypofractionated schedules) was mandated for node negative and encouraged for node positive disease. There were 1,974 patients randomized and over a median follow-up of 72 months (IQR 60–84), metastasis-free survival was significantly longer in the combination-therapy groups (median not reached, IQR NE–NE) than in the control groups (not reached, 97–NE; HR 0.53, 95% CI 0.44–0.64). The 6-year metastasis-free survival was 82% (95% CI 79–85) in the combination-therapy group and 69% (66–72) in the control group. Overall survival (median not reached [IQR NE–NE] in the combination-therapy groups vs not reached [103–NE] in the control groups; HR 0.60, 95% CI 0.48–0.73). The Kaplan-Meier curves for M0 high risk, M1 low risk, and M1 high risk are as follows:

Dr. Attard highlighted that in the M1 cohort of this study, looking at the tails of the Kaplan-Meier curves, 30%-40% of men that received standard of care + abiraterone/prednisone may not benefit from additional treatments, whereas ~10% of patients in the standard of care arm may not require ARPI at all. Ultimately, among ~50-60% of patients with low burden disease, it is likely that there will be better control with radiotherapy to the primary, however we are still awaiting results of the PEACE-1 trial reporting the results for radiotherapy.
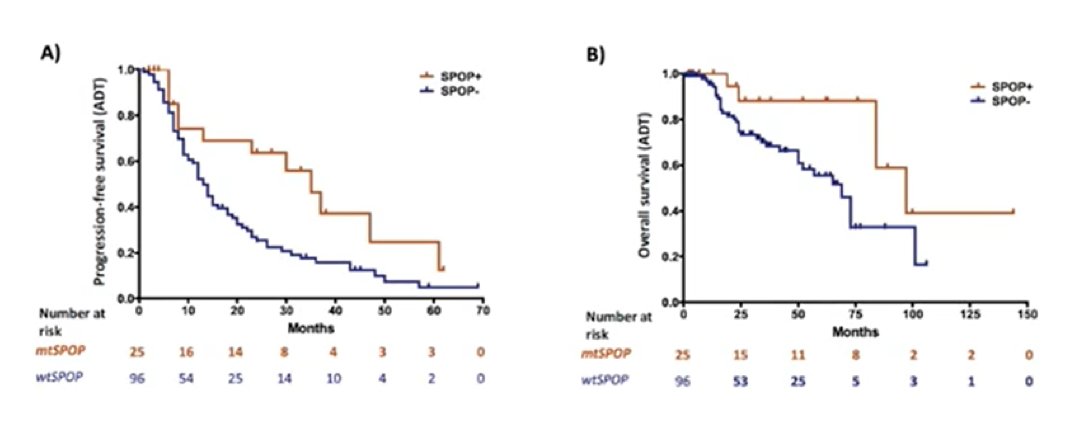
Swami et al.2 recently published the results assessing the association of SPOP mutation with outcomes in men with de novo mHSPC. Among 121 men (25 mtSPOP [21%] and 96 wtSPOP [79%]), mtSPOP was significantly associated with better median progression-free survival (35 vs 13 months; adjusted HR 0.47; p = 0.016) and overall survival (97 vs 69 months; adjusted HR 0.32; p = 0.027) after adjusting for covariates:
Prognostic biomarkers are also in development in the STAMPEDE trial. In work that has not yet to be published, copy number burden stratification has shown an association with prostate cancer specific mortality and Ki67 immunohistochemistry has shown an association with overall survival. To date, the effect of docetaxel does not appear consistent across disease states. In Dr. Attard’s view, the field needs a predictive biomarker for tailored docetaxel use, which would require a positive test of interaction between a biomarker negative defined group and docetaxel treatment. Early transcriptomic profiling work is hypothesis generating and may improve patient selection for docetaxel. Docetaxel + ADT versus ADT appears to improve overall survival and time to mCRPC in luminal B subtypes of tumors.
Dr. Attard concluded his presentation with a consensus view regarding biology and docetaxel selection, as well as ARPI selection:
- For docetaxel selection, evidence to aim for includes: (i) large independent sets from prospective trials analyzed using the same clinical assay and a pre-declared SAP that pre-specifies the magnitude and direction of docetaxel effect in molecular subgroups; (ii) prospective selection of treatment based on a test/timelines
- For ARPI selection, evidence to aim for includes: (i) a prognostic model trained and tested in large independent sets from prospective trials analyzed using the same clinical assay; (ii) prospective selection of treatment based on a test/timelines
Presented By: Gert Attard, MD PhD FRCP, University College London Cancer Institute, London, UK
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 Advanced Prostate Cancer Consensus Conference (APCCC) Annual Hybrid Meeting, Lugano, Switzerland, Thurs, Apr 28 – Sat, Apr 30, 2022.
References:- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022 Jan 29;399(10323):447-460.
- Swami U, Velho PI, Nussenzveig R, et al. Association of SPOP Mutations with Outcomes in Men with De Novo Metastatic Castration-sensitive Prostate Cancer. Eur Urol. 2020 Nov;78(5):652-656.