(UroToday.com) The 2022 Advanced Prostate Cancer Consensus Conference (APCCC) Hybrid Meeting included a session on the importance of lifestyle and prevention of complications in advanced prostate cancer, and a presentation by Dr. Fred Saad discussing how we should take care of our patient’s heart. Dr. Saad started his presentation by emphasizing that cardiovascular mortality is the leading cause of death in patients with prostate cancer.
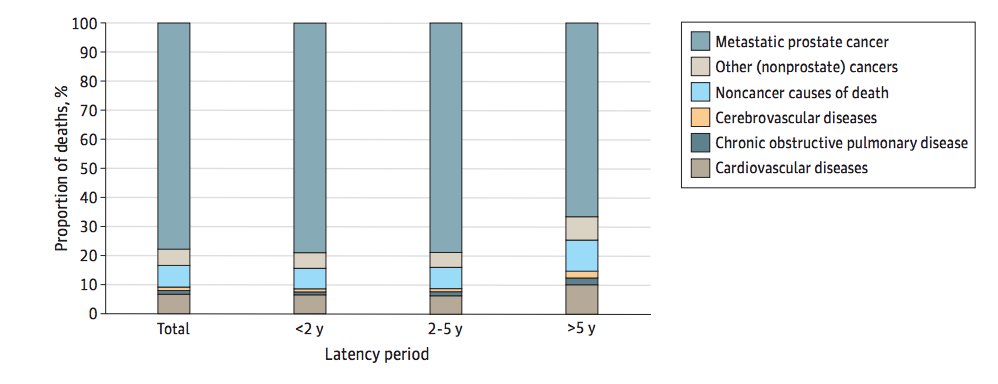
Additionally, it is important to remember that not dying from prostate cancer is a good thing, however as long as our treatment is not the cause of mortality. Additionally, there are competing risks for death even in men with metastatic prostate cancer. In a recent publication in JAMA Network Open, Elmehrath et al.1 found that non-cancer causes of death accounted for 16.7% of deaths, and cardiovascular disease accounted for 41.0% of these non-cancer related mortalities. Additionally, cardiovascular causes of death become even more important over time, with 35% of deaths not due to prostate cancer after 5 years:
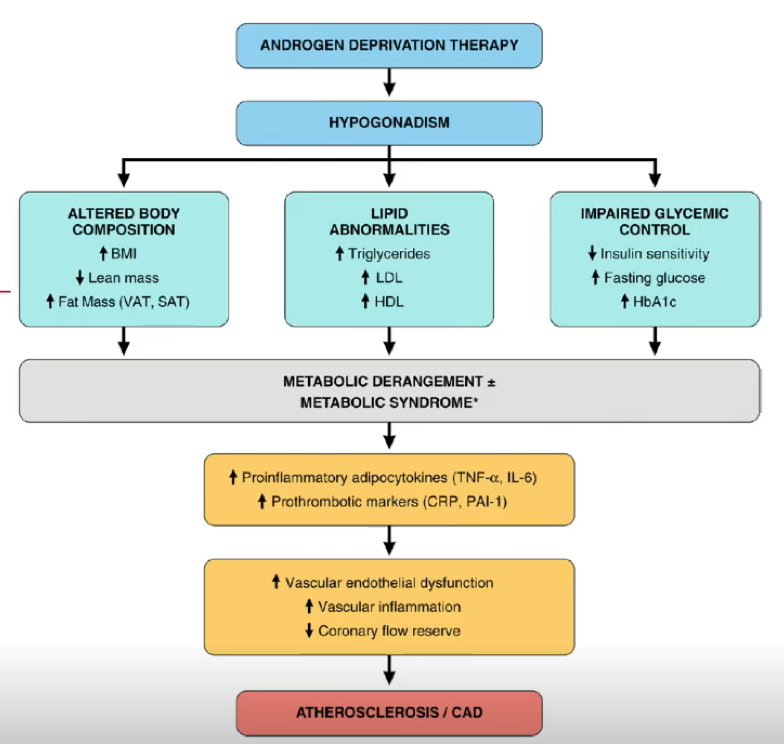
So, does ADT increase the risk of cardiovascular events? Dr. Saad this that yes, it probably does. However, there is poor consensus with regards to observational studies and RCTs delineating a true association between ADT and cardiovascular mortality. As follows is a proposed mechanism with a biological rationale for an association between ADT and cardiovascular mortality:
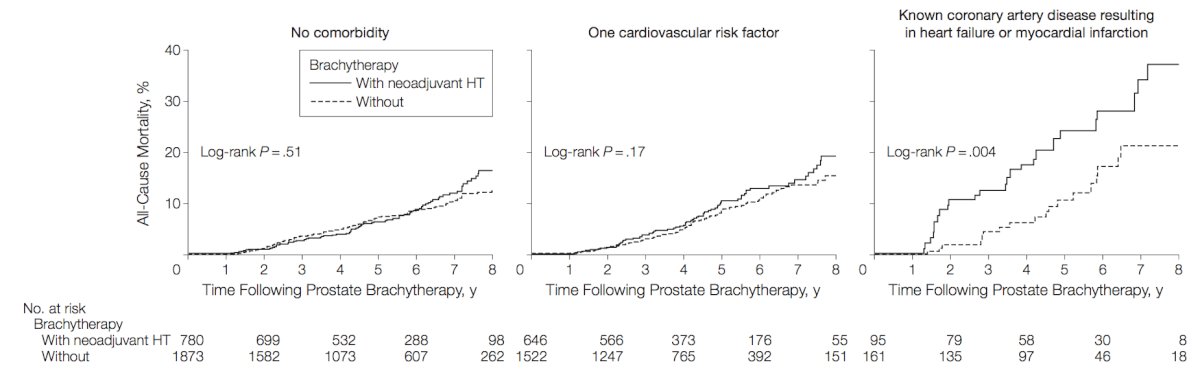
Work from the brachytherapy literature suggests that the presence of cardiac risk factors impacts risk of cardiovascular mortality with ADT. Nanda and colleagues2 assessed whether neoadjuvant hormonal therapy use affects the risk of all-cause mortality in men with prostate cancer and coronary artery disease (CAD)-induced congestive heart failure (CHF) or myocardial infarction (MI), CAD risk factors, or no comorbidity. Among 5,077 men with localized or locally advanced prostate cancer, neoadjuvant hormonal therapy use was not associated with an increased risk of all-cause mortality in men with no comorbidity (9.6% vs 6.7%, adjusted HR 0.97, 95% CI 0.72-1.32) or a single CAD risk factor (10.7% vs 7.0%, adjusted HR 1.04, 95% CI 0.75-1.43) after median follow-ups of 5.0 and 4.4 years, respectively. However, for men with CAD-induced CHF or MI, after a median follow-up of 5.1 years, neoadjuvant hormonal therapy use was significantly associated with an increased risk of all-cause mortality (26.3% vs 11.2%, adjusted HR 1.96, 95% CI 1.04-3.71):
Dr. Saad notes that one helpful mnemonic for assisting with the identification of patients with cardiovascular disease is ‘STAMP’:
- S – stroke
- T – transient ischemic attack
- A – abdominal aortic aneurysm or other aortic disease
- M – myocardial infarction, angina, or other previous revascularization
- P – peripheral arterial disease
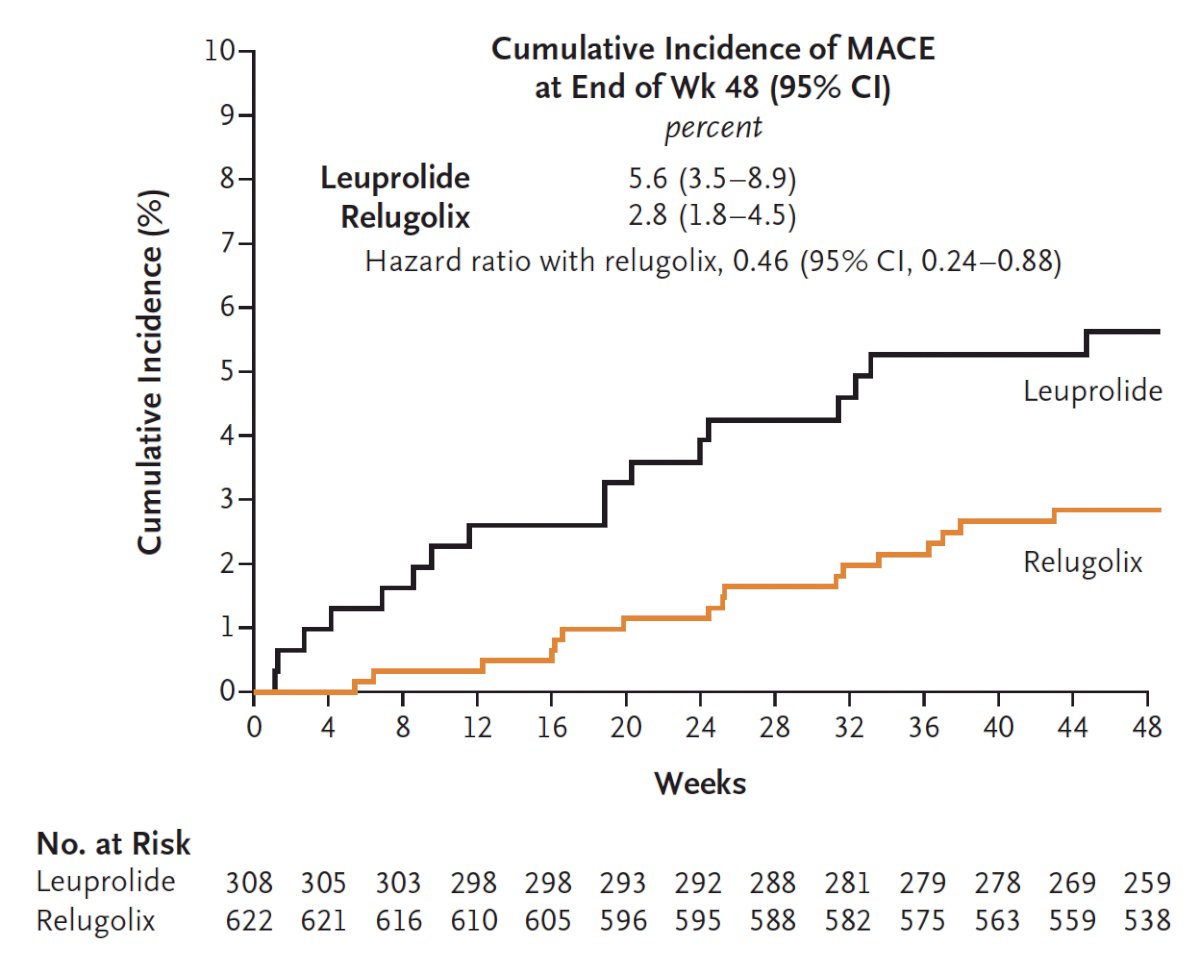
One of the most heated debates over the last several years is whether LHRH antagonists cause less cardiovascular risk than LHRH agonists. A meta-analysis from Cirne et al., that is not yet in print, encompassing 9 studies suggests that LHRH antagonists are associated with less cardiovascular events, with a relative risk of 0.46 (95% CI 0.22-0.96) compared to LHRH agonists. Work from the HERO trial3 assessing oral relugolix (an LHRH antagonist) for ADT in advanced prostate cancer showed that the cumulative incidence of MACE at the end of 48 weeks of treatment was 5.6% for leuprolide versus 2.8% for relugolix (HR 0.46, 95% CI 0.24-0.88), suggesting that relugolix decreased risk of MACE by 54%:
Furthermore, among men in the HERO trial with a history of MACE, the incidence of another MACE was 3.6% for relugolix and 17.8% for leuprolide.
However, these aforementioned findings are not consistent across the literature. A recent study assessing real-world cardiovascular outcomes associated with degarelix versus leuprolide found no significant difference in the risk of MACE for patients taking degarelix versus those taking leuprolide (10.18 vs 8.60 events per 100 person-years; HR 1.18, 95% CI 0.86-1.61). Degarelix was associated with a higher risk of death from any cause (HR 1.48, 95% CI 1.01-2.18) but not of myocardial infarction (HR 1.16, 95% CI 0.60-2.25), stroke (HR 0.92, 95% CI, 0.45-1.85), or angina (HR 1.36, 95% CI, 0.43-4.27).
The PRONOUNCE study was a randomized trial that assessed cardiovascular safety of degarelix versus leuprolide,5 with a primary outcome of time to first adjudicated MACE (composite of death, myocardial infarction, or stroke) through 12 months. Among 545 patients (planned enrollment was 900 patients), a MACE occurred in 15 (5.5%) patients assigned to degarelix and 11 (4.1%) patients assigned to leuprolide (HR 1.28, 95% CI 0.59-2.79). Cardiovascular events may have been lower in this study among men with prostate secondary to better awareness and attention to cardiovascular risk factor control.
Dr. Saad subsequently provided the ABCDE’s to reduce cardiovascular risk, highlighted as follows:
- A: awareness and aspirin/antiplatelet therapy (consider in higher risk patients)
- B: blood pressure (should be below 130/80)
- C: cholesterol (consider a statin – among men on ADT, decreased overall mortality by 27% and decreased cancer-specific mortality by 35%) and cigarettes (tobacco cessation)
- D: diet and weight management (BMI < 30, ideally <25) and diabetes prevention and treatment (possible role for metformin? Among men with prostate cancer, 28% improvement in OS, 22% improvement in CSS, and 40% improvement in RFS)
- E: exercise (150 min/week of weak/moderate exercise, or 75 min/week of intense exercise)
Dr. Saad concluded his presentation by discussing how to take care of the heart of our prostate cancer patients with the following summary messages:
- ADT associated with cardiovascular events and cardiovascular death in observational studies are not consistently reproducible in randomized clinical trials
- We should institute prevention strategies in all of our patients, including smoking cessation, exercise, and perhaps statins, aspirin, and metformin
- We need to identify patients with a cardiovascular history, using the STOMP assessment. For those that are moderate or high-risk we should involve other expertise (ie. cardiologist)
- It is unclear if there is a benefit of an LHRH antagonist over an LHRH agonist
As a final message, Dr. Saad emphasized that as our therapies for advanced prostate cancer become more effective and patients live longer with prostate cancer, taking care of the heart becomes even more relevant.
Presented By: Fred Saad, MD, FRCS, University of Montreal Hospital Center, Montreal, Quebec, Canada
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 Advanced Prostate Cancer Consensus Conference (APCCC) Annual Hybrid Meeting, Lugano, Switzerland, Thurs, Apr 28 – Sat, Apr 30, 2022.
References:- Elmehrath AO, Afifi AM, Al-Husseini MJ, et al. Causes of death among patients with metastatic prostate cancer in the US from 2000 to 2016. JAMA Network Open 2021;4(8):e2119568.
- Nanda A, Chen MH, Braccioforte MH, et al. Hormonal therapy use for prostate cancer and mortality in men with coronary artery disease-induced congestive heart failure or myocardial infarction. JAMA 2009 Aug 26;302(8):866-873.
- Shore ND, Saad F, Cookson MS, et al. Oral Relugolix for Androgen-Deprivation Therapy in Advanced Prostate Cancer. N Engl J Med. 2020 Jun 4;382(23):2187-2196.
- Wallach JD, Deng Y, McCoy RG, et al. Real-world cardiovascular outcomes associated with degarelix versus leuprolide for prostate cancer treatment. JAMA Network Open. 2021;4(10):e2130587.
- Lopes RD, Higano CS, Slovin SF, et al. Cardiovascular safety of degarelix versus leuprolide in patients with prostate cancer: The Primary results of the PRONOUCE randomized trial. Circulation. 2021 Oct 19;144(16):1295-1307.