(UroToday.com) The 2022 American Urological Association (AUA) Annual Meeting included a session on advanced kidney cancer and a presentation by Dr. Jun Teishima discussing a prognostic model of upfront cytoreductive nephrectomy in patients with metastatic renal cell carcinoma (RCC) treated with immune-checkpoint inhibitors and/or tyrosine kinase inhibitors. The aim of this study was to investigate prognostic factors and to establish a prognostic model using data from upfront cytoreductive nephrectomy patients with metastatic RCC treated with immune checkpoint inhibitors and/or tyrosine kinase inhibitor.
There were 400 patients with metastatic RCC treated with tyrosine kinase inhibitor and/or immune checkpoint inhibitors that were classified into 3 groups:
- Those undergoing cytoreductive nephrectomy (upfront cytoreductive nephrectomy group, n = 117)
- Those who initially underwent systemic therapy (non-upfront cytoreductive nephrectomy group, n = 94)
- Those whose recurrence was detected after radical nephrectomy (radical nephrectomy group, n = 189)
In the upfront cytoreductive nephrectomy group, patients’ background characteristics and overall survival (OS) were compared to those in the other two groups, and prognostic factors were analyzed. Subsequently, the prognostic model of upfront cytoreductive nephrectomy group was established.
The median follow-up period for the upfront cytoreductive nephrectomy group was 25 months. The number of patients with clear cell histology (87.2% vs 30.9%, p < 0.0001), Karnofsky performance status (KPS) ≥80% (92.3% vs 77.7%, p = 0.0025), single metastatic organ (41.9% vs 24.5%, p = 0.008), normal pretreated C-reactive protein level (7.9% vs 13.8%, p < 0.0001), and IMDC intermediate risk (66.7% vs 45.7%, p = 0.002) were significantly higher than those in non-cytoreductive nephrectomy group. The median OS in the upfront cytoreductive nephrectomy group was 33.1 months, significantly better than that in non-upfront cytoreductive nephrectomy group (11.1 months, p <0.0001), and these results were consistent regardless of prognostic risk level. Multivariate analysis showed that multiple metastatic organs (HR 1.65, p = 0.03) and KPS <80% (HR 2.99, p = 0.005) were independent predictive factors for overall survival. Using these two parameters to stratify the upfront cytoreductive nephrectomy group, the median overall survival for patients with no risk factors was 43.4 months, for those with one risk factor was 29.1 months, and for those with two risk factors was 7.7 months (p <0.0001):
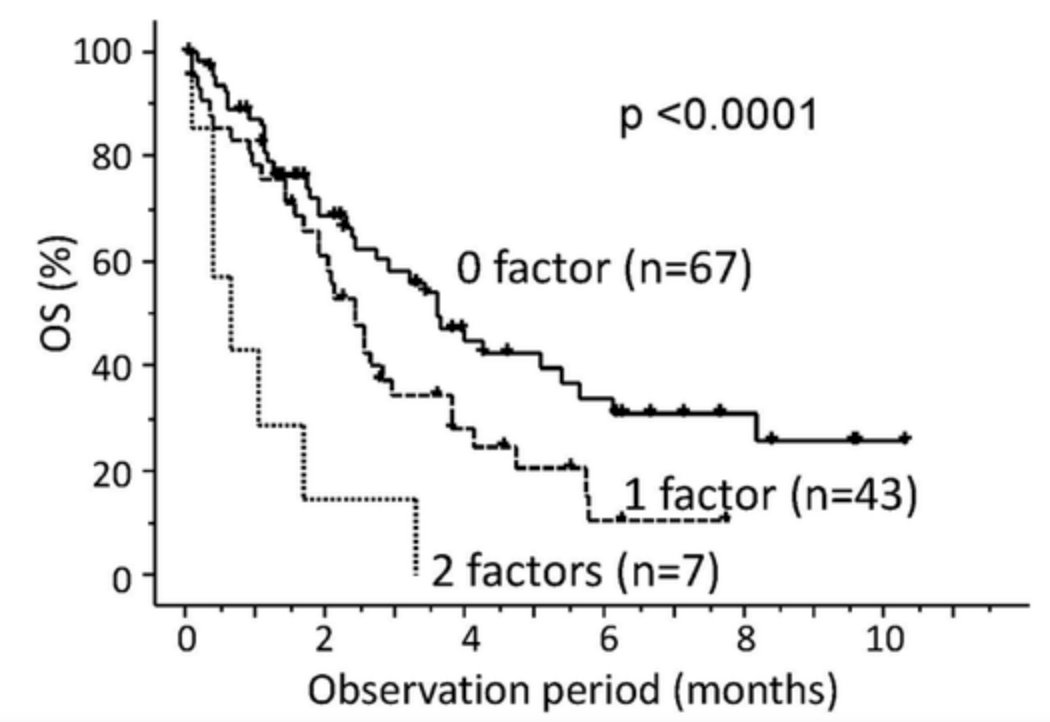
Dr. Teishima concluded this presentation by discussing a prognostic model of upfront cytoreductive nephrectomy in patients with metastatic RCC treated with immune-checkpoint inhibitors and/or tyrosine kinase inhibitors with the following concluding points:
- The upfront cytoreductive nephrectomy group is able to be stratified by our prognostic model into three subgroups with different prognosis
- This model can provide us with useful information for making a decision of considering upfront cytoreductive nephrectomy in patients with metastatic RCC
Presented by: Jun Teishima, Department of Urology, Hiroshima University, Hiroshima, Japan
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 American Urological Association (AUA) Annual Meeting, New Orleans, LA, Fri, May 13 – Mon, May 16, 2022.