- The supporting evidence is very poor
- The morbidity of treatment is increased
- Local progression is only a problem in a minority of patients
- Lessons from breast cancer
- First data from a randomized trial are available.
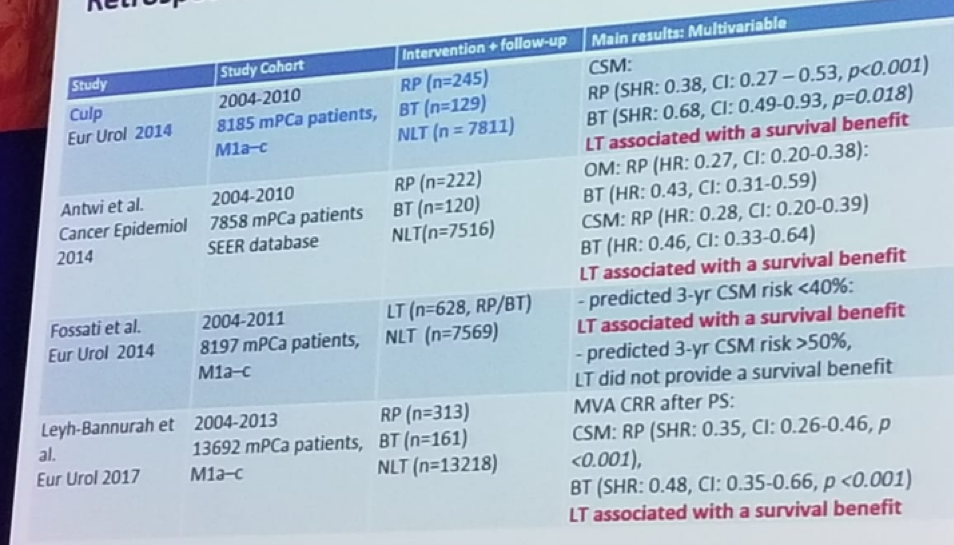
There is retrospective data, which is SEER database based, showing a benefit for local treatment in metastatic disease (Table 1). However, the SEER database has significant limitations including lack of information on comorbidities, no available codes on site-specific EBRT, there is no data available on post-treatment PSA values and data regarding systemic therapies, the metastatic extent is not known, and lastly, baseline PSA is only available from 2010 and onwards. There are additional retrospective data, including the Munich cancer registry, demonstrating a benefit for local treatment with a survival advantage.1However, the selection bias in these studies is very significant. The fundamental shortcomings of methods and unknown confounders make interpretation of these finding almost impossible. Men undergoing local therapy are more likely to be fit, have a lower burden of metastatic disease, have robust disease responses with systemic therapy. Therefore, there is no surprise these patients do better and may have probably done well without local treatment.
Table 1 – Retrospective SEER database data:
Next, Tilki discussed the topic of local control. In men with bone metastasis, death usually occurs before local progression. A relevant study demonstrated that 35% of men with bone metastases treated with androgen deprivation therapy (ADT) alone had local symptoms and required nephrostomy catheter/tubes/stents/ TURP.2
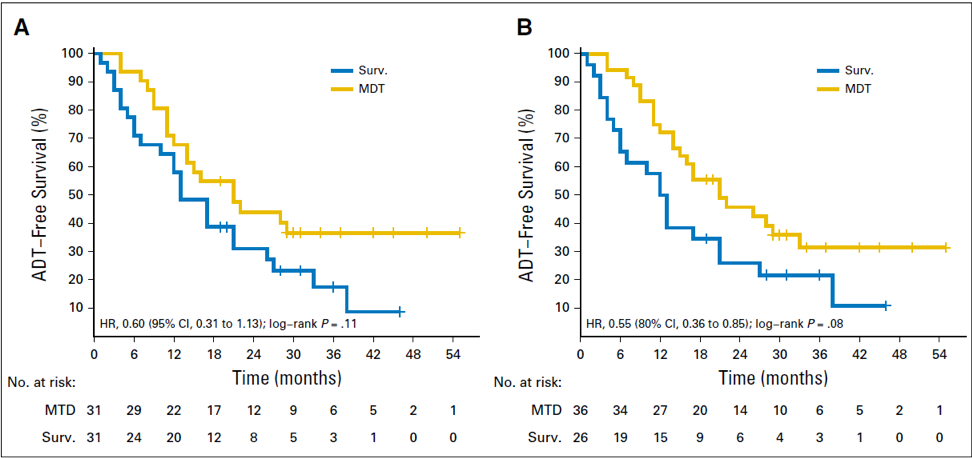
There are prospective randomized data available in breast cancer. This study in breast cancer showed no difference in overall survival (OS).3 In PC there is a randomized trial as well, examining the role of local therapy in the metastatic setting.4 This demonstrated that ADT-free survival was longer with local treatment than with surveillance alone for oligorecurrent PC, suggesting that local treatment should be explored further in phase III trials.
Figure 1: Kaplan-Meier plot comparing androgen deprivation therapy (ADT)–free survival of surveillance versus metastasis-directed therapy (MDT) for (A) the intention-to-treat analysis and (B) the per-protocol analysis:
In conclusion, despite this preliminary supporting data for local treatment in metastatic PC, administration of local treatment in this setting, according to Dr. Tilki, is not ready to be introduced into clinical practice. Currently, it is only to be considered as part of a randomized trial.
References:
1. Tilki et al. Int. J of Urol, 2018
2. Steuber et al. Eur Urol Focus 2017
3. Badwe et al. Lancet Oncol 2015
4. Ost P. et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J Clin Oncol. 2018 Feb 10;36(5):446-453. doi: 10.1200/JCO.2017.75.4853. Epub 2017 Dec 14.
Presented by: Derya Tilki, MD, Martini-Klinik, Hamburg, Germany
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the 2018 FOIU 4th Friends of Israel Urological Symposium, July 3-5. 2018, Tel-Aviv, Israel